


Vaccine Evangelists, Apostates, & Apologists – Part 7: The Apologist’s Playbook

This is the 7th and final installment of this essay series. Here is the itinerary of the final installment: It’s been a while since the publication of the 6th installment, so to get back in the rhythm of the series I’ll kick off this installment with some classic anti-vaccinationist fun – juxtaposing pro-vaccine propaganda with the reality that directly contradicts it.
We’ll look at how an illustrious Belgian institution attempts to deceive the reader into believing that Belgium’s 1959 routine diphtheria vaccination program is responsible for the plummet in Belgian diphtheria mortality, and then we’ll cure that fanciful pro-vaccine notion with a dose of reality.
Next I will sum up the principle strategies by which vaccine apologists attempt to dismiss the awkward little detail that the big, bold, pro-vaccine historical mortality-based messages are directly contradicted by the historical mortality data – this summary is the Vaccine Apologist’s Playbook.
Following the playbook will be a discussion of the implications of what we have studied in this essay series. I’ll also provide (in an appendix) suggested reading for other areas of the vaccine debate that this series hasn’t touched on at all due to these other areas lying outside the scope of this series.
For the finale I’ll close the series with a review of the Italian historical mortality data juxtaposed with vaccine introduction – the Italian mortality data is especially noteworthy for reasons that will be discussed momentarily.
First though, here are links to all the earlier essay installments of this series, followed by a table of contents for this essay installment.
Links to the earlier essay installments.
Part 3 - The Red Herring: A Tour of the Motte
Part 6 The Apologists Continued
Table of Contents for this Essay Installment
1. Belgian Diphtheria Vaccine Propaganda vs What Actually Happened
2. The Vaccine Apologist’s Playbook
Vax-Apologist Strategy #1 – Conflate historical arguments with efficacy arguments.
Vax-Apologist Strategy #2 – The no duh approach accompanied by unsubstantiated claims about medical care.
Vax-Apologist Strategy #3 – The argument from the data we don’t have.
Vax-Apologist Strategy #4 – The whooping cough warning story.
Vax-Apologist Strategy #5 – Pointing to that same, one, Canadian measles case notifications graph.
Vax-Apologist Strategy #6 – Direct defense of the narrative.
Vax-Apologist Strategy #7 – The Shameless Projection Gambit
3. Revelation of character and conduct
4. Important strategic consideration
5. Child mortality reduction, late vaccine introduction, and low vaccine coverage in Italy
Appendix: Further Reading & Resources
This article was originally published on Winter Oak, Activist Post, Nevermore, and Valerie Kochmann.
1. Belgian Diphtheria Vaccine Propaganda vs What Actually Happened
~
What They (Sciensano – Belgium’s Institute of Public Health) Would Have You Believe Happened in Belgium.
The following excerpts are from the diphtheria page on the website of Sciensano. Emphasis is mine:
“In the past diphtheria was a major cause of death among children. Thanks to widespread vaccination in Belgium since 1959, diphtheria has almost disappeared from our country. But the bacteria are still in circulation and vaccination is the only way to prevent diphtheria.”
“Thanks to widespread vaccination in Belgium since 1959, the number of cases has decreased considerably and the risk of a diphtheria epidemic is currently minimal.”
1943: 16,157 cases and 982 deaths
1980 – 2012: less than 15 cases and 1 death (a person of Belgian nationality in Moscow)
2013: 1 case of respiratory diphtheria due to a toxigenic strain of C.ulcerans
2014: 0 cases
2015: 3 cases of cutaneous diphtheria, 2 related to a toxigenic strain of C. ulcerans and 1 due to a toxigenic strain of C. diphtheriae
2016: 1 fatal case of respiratory diphtheria in a 3-year old unvaccinated child”
Sciensano leads with talking about death, and then they switch to talking about vaccination reducing cases. This allows them to strongly imply that vaccination is the reason for diphtheria no longer being a major cause of death in Belgium, while leaving themselves a very thin layer of plausible deniability.
Sciensano proceeds to tell us about the historical mortality data rather than just showing it to us. They give us the number of diphtheria deaths in 1943 (982 deaths) to illustrate the world before vaccines. Their message is clear enough, and can be summed up as so:
Diphtheria used to be a major cause of child mortality in Belgium.
Diphtheria is no longer a major cause of child mortality in Belgium.
Vaccination is the reason that diphtheria is no longer a major cause of child mortality in Belgium.
We’ll revisit their message in a moment.
What Actually Happened in Belgium.
Figure 60
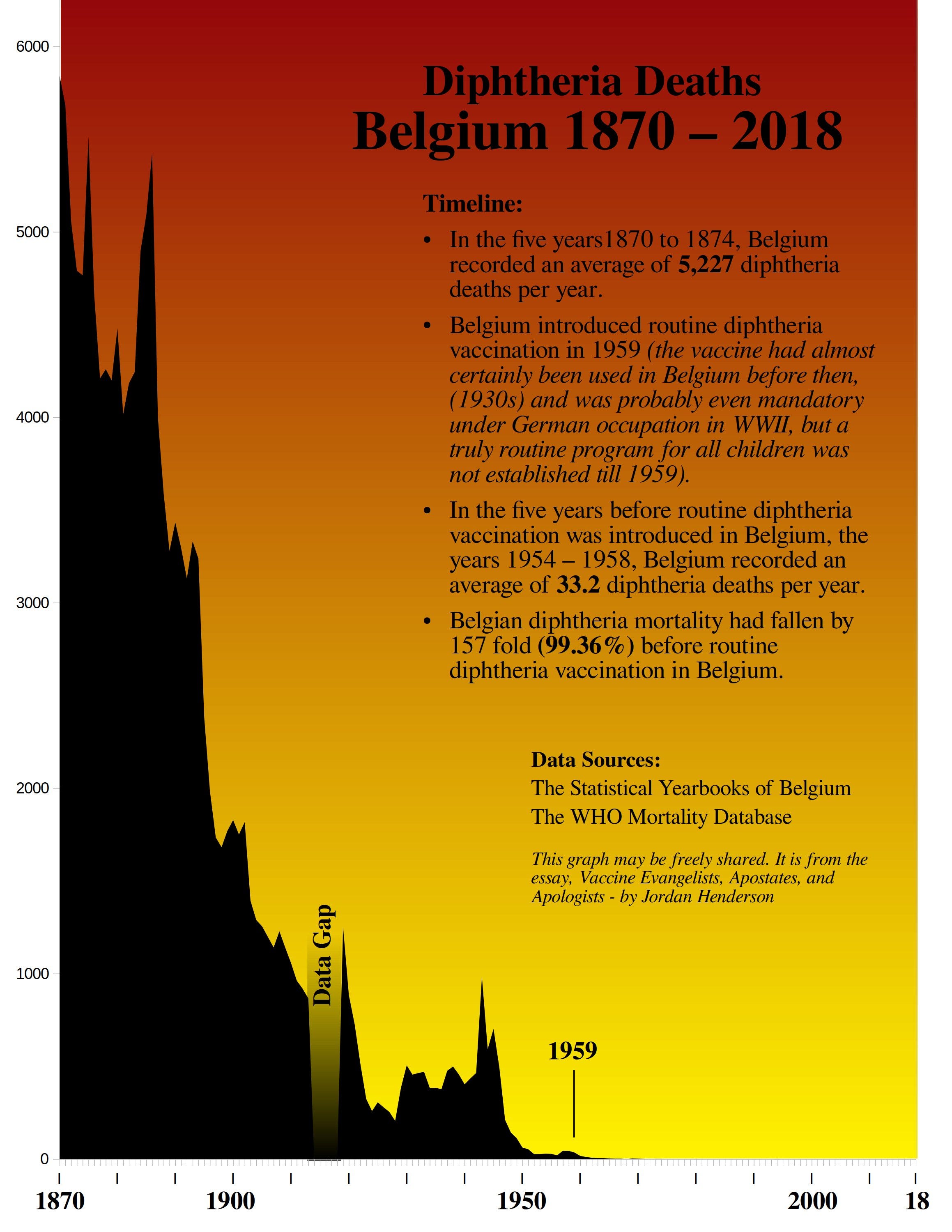
Even if one believes that diphtheria vaccinations are of any value at all, it is still inescapable that widespread diphtheria vaccination in Belgium in 1959 cannot be the primary reason for the diphtheria mortality decline, as almost all the decline occurred before 1959.
Sciensano only provides us the 1943 statistic of 982 deaths for pre-vaccine era historical perspective, yet still, it is unavoidable that widespread vaccination beginning in 1959 cannot be the principle reason for Belgium no longer having 900+ diphtheria deaths a year either, as most the post 1943 decline (95%) also occurred before 1959.
Sciensano’s vaccine propaganda uses the exact same two truths and a lie formula that we’ve seen the health authorities in the USA, Spain, and Ireland, using, and they do it for the same reason – to make it seem as if vaccination played the leading role in the historical reduction of infectious disease mortality.
The Basic Two Truths and a Lie Historical Mortality Formula for Promoting Vaccines is as Follows (the same formula works for other countries and illnesses):
Diphtheria used to be a major cause of child mortality in Belgium. = TRUE
Diphtheria is no longer a major cause of child mortality in Belgium. = TRUE
Vaccination is the reason that diphtheria is no longer a major cause of child mortality in Belgium. = FALSE
2. The Vaccine Apologist’s Playbook
Note: This playbook is intended as a resource for anticipating pro-vaccine responses when they have had their pro-vaccine historical mortality propaganda debunked. If you’re not planning on actively debunking pro-vaccine historical mortality based claims anytime soon, then you may not wish to study their responses in this much detail. Feel free to just skim through the playbook, stopping at what interests you and otherwise moving onto Section 3 of this essay – Revelation of Character and Conduct.
This playbook is based on field observations of the vaccine apologists in their natural habitats – from the wilds of the blogosphere, to the orderly pages of government documents. The 15 Vaccine Apologetics Case Examples documented and reviewed in Parts 3, 5, and 6 of this essay series are the principle basis from which I am drawing my observations for writing this playbook.
The vaccine apologists do regularly publish their own playbooks. For example, the Australian Government document, Responding to arguments against vaccination - a guide for providers (which we reviewed as Vaccine Apologetics Case Example 9 last essay), is a clear example of a playbook for vaccine apologists.
Case Example 5 from last essay, the CDC’s Some Common Misconceptions about vaccination and how to respond to them, is also a clear example of a playbook for vaccine apologists.
The vaccinationists are currently working on newer, better playbooks. For example, JitsuVax is an EU funded multi-university collaboration working on a slick, interactive, vaccine apologist’s playbook, designed to guide the apologist to the right answers to specific anti-vax talking points, and provide them with insight and guidance for responding to anti-vaccine arguments.
With so many literal vaccine apologist’s playbooks already out there, and the next generation of vaccine apologist’s playbooks in the works and already functional, what am I bringing to the table with another vaccine apologist’s playbook?
I’m bringing the one where the quiet parts are said out loud.
This playbook is more specialized, too; it’s centered solidly within this essay’s scope: the matter of vaccines being credited for what they did not do (credited as being the major reason for the historical infectious disease mortality declines).
Let’ recap the predicament the apologists are in.
Some of the most popular messages preached by the vaccine evangelists involve crediting vaccines for a large portion, up to most or all, of the infectious disease mortality decline from what it was in the early 20th and late 19th centuries to what it is now. (see Vaccine Evangelism Exhibits A through Z in parts 1, 4, and 7).
These are simple, easy to understand messages that powerfully illustrate the value of vaccines and help encourage the public to get vaccinated.
The difficulty for the vaccinationists is that these popular talking points of theirs are directly contradicted by the historical mortality data.
When people find this out, such as when vaccine apostates graph out the historical mortality data and show it to people, this undermines people’s faith in vaccines, and may prompt them to ask:
“If they’ve been misleading us on this aspect of vaccines, where else have they been misleading us? Have they been exaggerating the safety of the vaccines, and omitting crucial information there, too?”
This is where the vaccine apologists step in and assure everyone that really the vaccinationists haven’t been misleading anyone, and that it is really the anti-vaxxers who are being misleading by bringing this up at all, and that the historical mortality data doesn’t matter much to the vaccine discussion, and so forth.
Here are the ways they do that:
Vax-Apologist Strategy #1 - Conflate historical arguments with efficacy arguments.
In this strategy the apologist acts as though the primary or sole purpose of the anti-vaccine graphs and historical mortality based arguments is to show vaccines as inefficacious. The apologist points out that most mortality graphs don’t tell us much about vaccine efficacy. The apologist finishes with accusing the anti-vaxxers of being intellectually dishonest and logically fallacious. (See Figure 43 in Part 5, for more details on how this strategy works.)
The obvious usage of the graphs for testing pro-vaccine claims that directly relate to historical mortality data is simply ignored by the apologist. That the vaccinationists themselves promote vaccines with historical mortality based arguments is sometimes denied (such as Case Example 2), but most often just ignored.
~
How popular is this strategy? 12 out of the 15 Vaccine Apologetics Case Examples reviewed in this essay series used this strategy either as their main strategy or as an auxiliary strategy.
(The three that did not use this strategy were Case Examples 3, 4, and 7 – all the others used this strategy.
Case Examples 3, and 4 were direct defense of the narrative and so did not need to pivot to notifications.
Case Example 7 did pivot to case notifications, but instead of using conflation to do that they mostly used the argument from the data we don’t have, which we’ll look at in a moment.
Case Example 5 (CDC) makes no mention of graphs, but does of pre-vaccine declines which the CDC treats as being related to case notifications only, and so I have counted Case Example 5 as having used a variant of this strategy.)
Vax-Apologist Strategy #2 – The no duh approach accompanied by unsubstantiated claims about medical care.
When someone debunks a pro-vaccine historical mortality related talking point, the vaccine apologists of course want to avoid conceding that the anti-vaccinationists had a valid point, or that the vaccinationists had been deceptive. They do this by using the no duh approach to make it seem like the vaccinationists had never been trying to credit vaccines with most of the infectious disease mortality decline to begin with.
The apologist acts as if vaccines having had very little (if anything) to do with the historical infectious disease mortality declines is the sort of thing that would come as no surprise to anyone.
They treat it as brutally obvious that most of the mortality decline would have occurred without the vaccine. They don’t, of course, say that most of the mortality decline occurred without the vaccine, no not like that, instead they understate it by just saying that mortality rates were declining.
After this they often make the unsubstantiated claim that the pre-vaccine decline was because of medical care. If they offer any example to try to substantiate this it’s usually polio and the iron lung (see A close look at Gorski’s iron lung example from Part 5 of this essay series).
Sometimes they are more reasonable and mention some other factors such as nutrition, and living conditions too, but their preference is to make medical care out to be the main reason – often mentioning medical care only. Presumably because they don’t want people thinking that the disease had become far less of a threat. Better to keep people thinking of kids on scary life support systems as the main reason for the mortality decline. Make the possibility of a world without vaccines look dreadful.
~
How popular is this strategy? 9 out of the 15 Vaccine Apologetics Case Examples reviewed in this essay series used the no duh approach accompanied with unsubstantiated claims about medical care.
Those were case examples 1, 2, 5, 6, 7, 8, 11, 14, and 15.
Vax-Apologist Strategy #3 – The argument from the data we don’t have.
Here the apologists invoke the historical serious disease complications sorted by cause data that we don’t have, to downplay the historical serious disease complication sorted by cause data that we do have (death).
They point out that illnesses can cause all manner of other grave consequences besides death. They themselves don’t provide any such data that is comparable to the historical mortality data, they simply point out that the anti-vaxxers didn’t provide this data (which they can’t find either, but they don’t mention that).
After stressing the importance of serious disease complications to downplay death data, the apologist refocuses the conversation on case notifications. That case notifications are a far cry from serious disease complications data, they don’t acknowledge; they just act as if somehow case notifications have more to do with serious disease complications than does death.
Sometimes they round this out by using the anti-vaccinationist’s focus on mortality data instead of case notifications data as a reason for accusing the anti-vaccinationists of being heartless, callous people who don’t care about the suffering of children – the implication being that if they really cared about the suffering of children they would be more concerned with case notifications data rather than death.
~
How popular is this strategy? 5 out of the 15 Vaccine Apologetics Case Examples reviewed in this essay series argued from the data that we don’t have.
Those were case examples 1, 2, 7, 14, and 15.
Vax-Apologist Strategy #4 – The whooping cough warning story.
To give the impression that without vaccines mortality rates would soar, the apologist invokes the whooping cough warning story. Usually this involves pointing to what happened in Sweden, the UK, and Japan when pertussis vaccination rates in those countries fell.
Unfortunately for the vaccinationists, in most places where the pertussis vaccination rates fell, so also did pertussis mortality, or it stayed low, which contradicts the message they want to push. They can talk about case notifications going up, but as always they need something much more frightening and impactful; they need to make it seem like mortality went up too.
To give the idea that mortality went up, rather than down or stayed the same, they either use Japan mostly and imply that the same thing happened in the UK and Sweden, or they simply mention the deaths that occurred in the UK after vaccination rates fell and act as if it was more than when vaccination rates were higher.
~
How popular is this strategy? 4 out of the 15 Vaccine Apologetics Case Examples reviewed in this essay series used the whooping cough warning story.
Those were case examples 2, 3, 5, and 9
Vax-Apologist Strategy #5 – Claim that anti-vaccine historical mortality graphs are in general dishonest, then point to that same, one, Canadian measles case notifications graph.
Pretty self explanatory: The apologist begins by claiming that anti-vaccine historical mortality graphs are in general intellectually dishonest. Then if they want to appear as if they actually have a basis for this claim they need something to point to.
Unfortunately for the vaccine apologists they don’t have many examples of anti-vaccine graphs that are actually intellectually dishonest. In fact the only example I see them point to that really is intellectually dishonest, isn’t even a mortality graph at all. It’s that same, one, Canadian measles incidence graph covered in the 2010 Gorski article (which we reviewed in this essay series as part of Case Example 2, in Part 5).
No matter – the apologists need something to point to. If they can only think of one example which isn’t even a mortality rate graph, then they make do with what they have. Most readers won’t conduct a study of 15 different examples of this kind of vaccine apologetics as we have done and will therefore not know that the apologists who make this claim about anti-vaccine historical mortality graphs are all pointing at the same anomalous example as their “representative” example.
~
How popular is this strategy? 4 out of the 15 Vaccine Apologetics Case Examples reviewed in this essay series claimed that anti-vaccine historical mortality graphs are in general intellectually dishonest, and then backed this up by pointing to that same Canadian measles case notifications graphs (by citing Gorski).
Those were case examples 2, 6, 7, and 12
Vax-Apologist Strategy #6 – Direct defense of the narrative.
This is a strategy for only the most daring of the vaccine apologists. It does not involve trying to reroute the conversation to notifications data, nor do the audacious apologists who attempt direct defense worry about gaslighting their audience into forgetting about the big, bold, historical mortality related pro-vaccine claims.
No, none of that: these apologists attempt to directly defend the claims that their fellow vaccinationists have been making.
There is simply no easy way for them to do this. Foolhardy bravery notwithstanding, the direct defense is untenable if subjected to any serious scrutiny.
The Irish health board (Case Example 3) relied on the public’s unfamiliarity with logarithmic scales to attempt the direct defense. I’m sure they fooled plenty of unsuspecting parents, but it must not have worked too well as I don’t see them trying it now.
Ian A. York (Case Example 4) fabricated a data point and left out a half century of data in his attempt at direct defense. That backfired just about immediately and he was backtracking in no time.
The Australian government health agency (Case Example 9) was a little more clever using a hybrid strategy of rerouting the conversation to case notifications data, but then still attempting a direct defense later using their own historical mortality graphs. In these they provided as little of the relevant information as they could get away with while still trying to prop up the pro-vaccine historical mortality related beliefs.
~
How popular is this strategy? 3 out of the 15 Vaccine Apologetics Case Examples reviewed in this essay attempted to directly defend the belief that vaccines played the major role in the infectious disease historical mortality declines.
Those were case examples 3, and 4 (direct defense as primary strategy) and 9 (hybrid strategy incorporating some direct defense).
Vax-Apologist Strategy #7 – The Shameless Projection Gambit
I call this the shameless projection gambit because it is an attempt to get the attention away from the fact that vaccinationists regularly hide/omit information by accusing the anti-vaccinationists of hiding information, whenever they (the anti-vaccinationists) reveal what the vaccinationists have hidden.
It is the vaccinationists who regularly omit the “detail” about almost all the mortality decline for various infectious diseases having occurred pre-vaccine, or without a vaccine at all.
When anti-vaxxers expose this by showing people the big picture, the vaccine apologist first concedes that the maximum theoretical contribution of vaccines to the mortality decline is so little as to be unnoticeable in the big picture (they don’t say it so plainly though), then they use this as the basis for accusing the anti-vaxxers of being the ones who are hiding something (by showing what the vaccinationists have been omitting).
The apologist insists that the only reason the anti-vaccinationists are showing you the big picture is to hide the alleged contribution of the vaccine. Like this:
“This is the problem with the anti-vaccine graph, it is deliberately zoomed out so far that you can’t see the impact of vaccines. That is why the pro-vaccine graph is a better representation. It’s not zoomed in as an effort to conceal something, rather it is zoomed in because that is the only way to see that vaccines did actually have an important impact.” From the article Yes, vaccines did save us from disease: a graphic analysis (which we reviewed last essay as Vaccine Apologetics Case Example 11)
So this strategy is an add on to the no duh approach. The apologist acts as though it is already well known that the maximum theoretical contribution of vaccines to the mortality decline was so little as to be unnoticeable in the big picture and that therefore the only reason to show the big picture is to hide the theoretical contribution of vaccines.
They avoid seeing the obvious usage of the graphs for debunking vax-evangelist historical mortality based claims, by, as usual, simply not acknowledging that their fellow vaccinationists have been preaching the messages that they preach.
~
How popular is this strategy? 2 out of the 15 Vaccine Apologetics Case Examples reviewed in this essay series used the shameless projection gambit and accused anti-vaccine graphs of hiding the impact of vaccines because they showed the big picture.
Those were case examples 6, and 11.
While the “net” I cast of 15 Vaccine Apologetics Case Examples only picked up two instances of this strategy, I’ve seen this strategy crop up elsewhere. Here is a very clear example: Melanie Mallon used the shameless projection gambit in her 2015 article The TRUTH about Bad Measles Charts the Mainstream Media Is Suppressing published on SkepChick.
She looked at a graph which showed that nearly 100% of the measles mortality decline in England had occurred pre-vaccine and stated:
“There’s only one reason to start this graph in 1838: to increase the scale so that the death rate appears even smaller in the years before the vaccine was introduced than it would if the graph focused on a relevant time frame. It’s not like anyone looking at this doesn’t already know that mortality from all causes was much higher in the 19th century than in the 20th.”
That’s a good case of shameless projection combined with the no duh approach. She in effect insists that it would come as no surprise to anyone to learn that the maximum theoretical contribution of the vaccine to the measles mortality decline in England is a fraction of a percent. Therefore according to Mallon, the only reason to look at the big picture is for the purpose of burying the fraction of a percent that represents the maximum theoretical contribution of the vaccine.
Note: I didn’t include Mallon’s article as a case example of vaccine apologetics because she doesn’t appear to have ever read the article that she is criticizing and doesn’t know what it’s title is. If you care to know how I know this here is a brief explanation – (otherwise just scroll on down to the debunk of the shameless projection gambit).
Malon says (emphasis mine):
“Roman Bystrianyk and Suzanne Humphries have a cherry to pick with proponents of vaccination. Their article on the measles vaccine was recently published on Health Impact News’s Vaccine Impact website under a heading promising us a mouthful of impacted truth: The Truth About Measles the Mainstream Media is Suppressing.
The actual article by Bystrianyk and Humphries is titled “Was the Introduction of the Measles Vaccine Responsible for Wiping Out Measles?” although the article barely even touches on that question, which is related to incidence of measles. Instead, the authors begin with a focus on mortality rates, which makes sense if you believe vaccines fight death, not disease.”
Mallon’s basic statements about the article she is criticizing are incorrect.
The original article is not titled “Was the Introduction of the Measles Vaccine Responsible for Wiping Out Measles?” That is a subheading on the Health Impact News article. The actual article is titled Vaccines: a peek beneath the hood.
The article begins with a focus on mortality rates, because vaccine proponents invoke mortality to illustrate the value of the vaccines. Bystrianyk and Humphries documented examples of historical mortality based vaccine evangelism at the beginning of their article. Mallon either never read the introduction of the article or pretends not to have.
Health Impact News did not publish Roman Bystrianyk and Suzanne Humphries’ article, they only published an excerpt of it – they cut the entire original introduction.
The article is not about measles vaccines specifically as Mallon claims. It is about vaccines in general with whooping cough, measles, and scarlet fever as case examples.
Mallon does have a valid point against the Health Impact News subheading, just not against the actual article. The Health Impact News’ article used an inappropriate subheading, and butchered the Bystrianyk and Humphries article by leaving out the article’s introduction which set the stage and provided key evidence.
Why did Mallon claim that the Health Impact News’ subheading was the actual article’s title? Most likely because she never followed the links back to the original article, or she pretended not to have. If she didn’t follow the links back then she wouldn’t have read the article’s introduction and would never have seen the actual title or key evidence presented by the authors.
Mallon’s sloppy journalism didn’t stop there. For example: she confidently asserted and insisted, citation free, that England did not introduce the measles vaccine in 1968 but instead in 1963. She really should have cited a source because the UK government certainly seems to think it was 1968.
In sum, Mallon’s article is a great example of the shameless projection gambit following the no duh approach. However, no matter what one thinks about vaccines, Mallon’s article is fatally flawed for the reason that she never read, or pretends to have never read, the whole article that she was critiquing, doesn’t know it’s title, doesn’t know what it’s actually about having missed the intro, and apparently didn’t realize this. I wasn’t sure what to do with something that sloppy so I left it out of the case examples.
Brief interlude to debunk the Shameless Projection Gambit.
These claims that the only reason to show the whole data set is to hide the theoretical contribution of the vaccine, can be easily debunked in a couple different ways. So let’s take a moment to do that.
The first way to debunk the Shameless Projection Gambit is to simply point out that because vaccine evangelists regularly invoke the pre-vaccine era in the 19th and early 20th centuries to illustrate the world before vaccines, then we have to show the whole data set reaching back into the 19th and early 20th centuries in order to thoroughly debunk those claims, and illustrate just how detached from reality those pro-vaccine messages are.
A second way to debunk the Shameless Projection Gambit is this:
Pro-vaccine advocates who want to maximize the impression of the vaccine’s contribution also use entire data sets going back deep into the 19th century. This establishes beyond doubt that there are other reasons to use the whole data set besides supposedly hiding the alleged contribution of the vaccines.
Ian A. York’s pro-vaccine post Measles deaths, pre-vaccine (Case Example 4) used an English measles mortality graph that goes all the way back to 1838.
The Irish health board’s Vaccination - Your Child's Best Shot” section of their MMR Information Pack (Case Example 3) used a graph of the Irish pertussis mortality that goes all the way back to 1864.
The Australian Government’s – Responding to arguments against vaccination - a guide for providers (Case Example 9), tried to make it seem as though they had provided as much historical perspective as they could.
Why then do some vaccine apologists, including government agencies, use the entire data set, or at least pretend that they have, while other vaccine apologists insist that only anti-vaxxers would do that? It simply depends on this:
If they are trying to defend what their fellow vaccinationists are actually preaching, then they need to make it look as though vaccines played a major, preferably foremost, role in the historical mortality decline.
On the other hand, if they have decided that they simply can’t pull off a direct defense of the misconceptions that their fellow vaccinationists have been preaching, then they need to act as if their side hasn’t been, and isn’t, making such claims to begin with, and gaslight their audience into believing that these claims are not being made.
At a Glance Summary and Prevalence in Percentages
Presented below, based on our 15 Vaccine Apologetics Case Examples, are the seven most common vaccine apologist strategies used to counter anti-vaccinationists who have debunked the pro-vaccine historical mortality related messages (such as the messages in Exhibits A through T in parts 1 and 4). Listed here is the percentage of case examples in which each strategy showed up.
80% – Conflated historical arguments with efficacy arguments
60% – Used the no duh approach accompanied by unsubstantiated claims about medical care.
33% – Employed the argument from the data we don’t have.
27% – Invoked the whooping cough warning story.
27% – Pointed to that same, one, Canadian measles case notifications graph.
20% – Attempted direct defense of the narrative.
13% – Used The Shameless Projection Gambit
That concludes the Vaccine Apologist’s Playbook.
3. Revelation of character & conduct
The study of the vaccine evangelist messages (Exhibits A through T in parts 1 and 4) that we have conducted in this essay series reveals that the vaccine advocates’ standard approach is to tell us whatever they think that we need to hear in order to convince us to do what they think that we should do – get vaccinated, and support vaccination.
We have seen that we cannot count on them to tell the truth and furnish us with the most relevant information; we can only count on the vaccinationists to tell us information that makes vaccines look good. We can also predict that no matter how relevant and critical certain information may be, they will omit that information if it looks bad for the vaccines, and if they can get away with omitting it.
The vaccine evangelist messages are so far removed from reality that most of the vaccine apologists do not even attempt to defend them and instead spend all their time rerouting conversations, conflating distinct ideas, engaging in shameless projection, gaslighting, and even going so far as to outright deny that their side has been preaching the messages that they are still preaching (Gorski in Case Example 2, Part 5. of this essay series).
Firm Grounds for Distrust
Most of us, myself included, do not have the time, means, and relevant expertise to put to the test every single one of the myriad claims and pronouncements made by the vaccinationists, but most of us can test at least some of those claims. We have done that. In this study of the vaccinationists (this essay series), we have tested their powerful historical mortality related claims (their Graveyard Gambits, and Lifespan Lectures, and Bait and Switch preaching).
We tested them; they failed. Furthermore, we know that they will generally not admit wrongdoing on their side, even when it has been firmly demonstrated. The apostates caught them red handed, and debunked their messages fair and square. The vaccinationists did not acknowledge their error and course correct. They instead responded by closing ranks, plowing ahead, and doing what they could to make the messenger (anti-vaccinationists) look like the villain.
Therefore we not only have good reason not to trust the pronouncements of vaccine experts – the pediatricians, immunologists, public health authorities, and so forth – but knowing what we know, it would be unreasonable and irrational for us to take them at their word.
Not being able to test the experts in a certain area is no reason to trust them – that would be an argument from ignorance. Consequently, even when we do not have the time, or do not have the means or expertise, to put to the test a vaccinationist claim, we nonetheless are fully justified in doubting the vaccine expert’s pronouncements, because:
The cumulative evidence of widespread deception on the part of vaccine experts and advocates is enormous. That presented in this essay series alone is sufficient grounds for strong distrust.
The takeaway lesson I see is this: when we do not have time or means to test a vaccine claim from authoritative sources like government health agencies, prominent vaccine developers, and doctors, we must rely on our knowledge of the character and conduct of the vaccinationist camp from the instances in which we could put them to the test. When we did put them to the test, such as we did in this essay series, we found that they are deceptive, omit critical information, and do not admit their wrongs when challenged but instead close ranks against the critics.
Rigging the risk benefit analysis
When vaccine advocates tell us whatever they think that we need to hear in order to convince us to do what they think that we should do (get vaccinated, and support vaccination), they are feeding the public information that in effect rigs people’s informal risk benefit analysis to ensure that people’s risk benefit analysis comes down solidly in favor of vaccines. They do this by making the alleged benefits of vaccines seem as great as possible while making the risks seem as small as possible.
People “know” that without vaccines we would see our local cemeteries crowded with ever more tiny headstones as our children drop dead to the scourges of the Victorian era. We would see our lifespans shortened by decades. The air would fill with dreadful sounds of children gasping for their last breath as they succumb to whooping cough, and diphtheria.
If people swallow the pro-vaccine historical mortality related claims and believe that vaccines really are the reason these illnesses don’t strike us the way they did in the 19th and early 20th centuries, then the benefit side of vaccines is stacked so heavily you might as well not even bother weighing the risks.
When it comes to exaggerating the alleged benefits of vaccines, the vaccinationists certainly don’t leave all their eggs in one basket. Wherever they can, they say whatever they can get away with, to stack the benefit side of the vaccine risk benefit analysis as high as possible. We’ve seen this with historical mortality related claims. I’ll provide you with another example of them doing this to illustrate my point further.
Measles vaccines saved 17 mill . . . wait, no – 56 million lives! – The impressive exponential growth of the simulated number of lives saved by measles vaccination!
The CDC on their webpage Fast Facts on Global Measles, Rubella, and Congenital Rubella Syndrome (CRS) Flatly state:
“Measles vaccines saved more than 57 million lives worldwide between 2000-2022.”
The WHO makes this statement in fact sheets too.
“Measles vaccination averted 56 million deaths being between 2000 and 2021”
&
“Accelerated immunization activities by countries, WHO, the Measles & Rubella Partnership (formerly the Measles & Rubella Initiative), and other international partners successfully prevented 56 million deaths between 2000–2021.”
That’s from the WHO’s measles Fact sheet.
The CDC and WHO both state this impressive number of 56 to 57 million lives saved like it’s a fact, on webpages called Fast Facts, and Fact Sheet. That kind of gives the impression that this statement is a fact, doesn’t it? Well it isn’t. The 56/57 million number is generated by running a simulation on a model. They’ve been generating impressive sounding numbers of lives saved by running simulations on models for years.
In order to generate more and more impressive sounding numbers they keep inflating the hypothetical number of deaths that they think there would have been in a no vaccine scenario. Take a look at some of their simulations:
Just a few years back their measles vaccine simulations generated 1.2 million lives saved per year. Between 2000 and 2014 measles vaccination saved an estimated 17.1 million lives!
Now measles vaccine simulations are generating a remarkable 2.7 million lives saved per year. Between 2000 and 2021 measles vaccination saved an estimated 56 million lives!
What is going on here? How did we go from 17.1 million lives saved by the measles vaccine between 2000 and 2014, to 56 million between 2000 and 2021?
Were an additional 39 million lives saved by the measles vaccine in just 7 years? For 14 years from 2000 to 2014 the measles vaccine saved an average of 1.2 million lives each year, and then after 2014, it saved on average 5.6 million lives, bringing us up to 56 million by 2021?
No, they just inflated the hypothetical number of measles deaths that they say there would have been in a no vaccine scenario across the entire time period (back to 2000), yielding for them a larger simulated number of lives saved for every year in their simulation.
Surely they can’t just “revise” their simulation to get as big of a number as they think the public is gullible enough to believe? They can. They can say whatever they want, because it’s all hypothetical.
Not only is the number of deaths that there would have been without measles vaccination unknown, the number of deaths that there were with measles vaccination is also unknown.
In contrast to England and Wales, Ireland, Australia, the USA, Belgium, Sweden, and Spain, that we have reviewed, most countries do not, and have not, kept detailed cause of death records. In the 2005 WHO Bulletin Counting the dead and what they died from: an assessment of the global status of cause of death data the authors found that:
“At the end of 2003 data on death registration were available from 115 countries, although they were essentially complete for only 64 countries. Coverage of death registration varies from close to 100% in the WHO European Region to less than 10% in the African Region.”
Even in 2021 UNICEF notes that still:
“Only about 60 countries, mainly high-income, have a well-functioning Civil Registration and Vital Statistics System which produces timely, high-quality mortality data.”
There are over 190 countries, so to this day we’re only looking at about a third of the world’s countries having this data.
This lack of data is a major advantage to Vax-Evangelists preaching globe spanning (as opposed to country specific) messages about lives saved and deaths averted by vaccination. They don’t have to worry about being contradicted by the hard data . . . because no one has it.
(Greg Beattie covered the early versions of these measles vaccine simulations in his book Fooling Ourselves on the fundamental value of vaccines. He also generously provided this chapter from his book as an article online which you can access over at TheRealAustralianSceptics, and I highly recommend reading it, as he covers aspects of their simulations that I won’t be covering here.)
These numbers, generated from simulations, run on models, are as far from factual as you can get. But the CDC and WHO present these numbers as though they are facts.
This supports my contention that vaccinationists will usually say whatever they can get away with saying to make vaccines look as good as possible. Presenting these impressive hypothetical numbers as though they were facts looks very good for vaccines.
Measles vaccines save X number of lives circular reasoning
The measles vaccine simulator generated numbers of 17 to 57 million lives saved are regularly trotted out as evidence of the vaccine’s global beneficial impact by Vax-evangelists and apologists alike. Even when vaccinationists acknowledge that the number is an estimate, they are engaging in circular reasoning if they use it as evidence of the vaccine’s alleged beneficial impact, because the simulation involves the assumption that the vaccines have had the intended impact.
Vaccination data is one of the data types they are using in their simulation. They say that right in the paper:
“The measles mortality model used to generate estimated measles cases and deaths is rerun each year using the new and revised annual WHO-UNICEF estimates of national immunization coverage data as well as updated surveillance data.”
You do not need to know how many people got vaccinated in order to estimate measles mortality unless you are using the vaccination data as part of your equation by making assumptions about the effectiveness of the vaccines. If you do that, then you can’t use your estimate as “evidence” of the vaccine’s impact because you just assumed what the real world efficacy of the vaccine is as part of your equation.
If we dig into their references for their model we find further confirmation of this (emphasis mine):
“The first routine dose of measles vaccine was assumed to be administered at 1 year of age, and we assume 85% efficacy. The second routine dose of measles vaccination was assumed to be administered to children at 2 years of age with 95% efficacy. The supplemental campaigns vary in the age groups targeted but are assumed to have 100% efficacy,”
That’s from their 3rd reference, the paper Estimation and prediction for a mechanistic model of measles transmission using particle filtering and maximum likelihood estimation
In sum, the measles vaccination simulator generated numbers prove a grand total of nothing about how many lives, if any, measles vaccines have saved. What they do serve as supportive evidence for though, is that the vaccinationists are so intent on rigging the risk benefit analysis in favor of vaccines that both of the world’s highest profile health institutions (The WHO and CDC) will go so far as to present hypothetical numbers as facts in their fact sheets.
4. Important Strategic Consideration
I stated early on in Part 2 of this series:
Death-rate graphs are only one of many types of evidence in the vaccine debate, but they will be the fulcrum of my analysis of the vaccine conflict, because death-rate graphs more succinctly illustrate, better than any other tool I know of, the disconnect between what the Vaccine Evangelists’ claim or imply happened, versus what actually happened.
This essay series sprang initially, in large part, from my identifying the need for a cleanup exercise to remove obstructions and pave the way for the unencumbered use of death rate graphs for debunking Vax-evangelist messages. The cleanup I saw a need for was to gather up, study, and dissect all the most common pro-vaccine attempts at dismissing death rate graphs.
If you are considering engaging in the good work of spreading vaccine realism, for the benefit of your friends, family, and/or audience (if you are a writer or podcaster), debunking the pro-vaccine historical mortality based messages is an excellent place to start.
Based on my observations of the vaccine debate itself, I’ll offer a recommendation on something to do first, before presenting the historical mortality data.
First document the position of the goal posts, then kick the ball
We know that most anytime anti-vaccinationists debunk the vaccinationists fair and square, the vaccinationists will simply pick up the goal posts, reposition them somewhere else, often in a completely different field, and then insist that the anti-vaccinationists don’t have a valid point because, look, see, the goal posts are way over there now.
What else are the vaccinationists going to do? Admit that their side has been deceptive and/or deluded in their beliefs? Admit that the the anti-vaccinationists were right? Of course not.
Even when you are simply in a personal discussion with a friend or family member, and have done your best to keep the discussion non adversarial, remove your ego from the discussion, and avoid confrontational wording that might inadvertently bring their ego into the discussion, there is still a good chance that they will move the goal posts on you anyway.
In my experience, belief in vaccination is strong enough that the believers generally evaluate the quality of the evidence based on how well it corresponds to their vaccine beliefs. If the evidence undermines their beliefs, then they “know” it must be wrong.
If they can’t demonstrate the evidence to be wrong, and it becomes clear to them that it is solid evidence, then the remaining option for them to prevent the evidence from undermining their belief is to “know” that it is irrelevant. The easiest way for them to know that it is irrelevant is to simply move the goal posts into another field where that evidence doesn’t apply.
This is why it is generally best to first document where the goal posts are positioned and who put them there, then kick the ball.
Many vaccine skeptics have already taken care to do this: Beattie opened his book Fooling Ourselves on the fundamental value of vaccines with a detailed example of the vax-evangelist’s Graveyard Gambits. Bystrianyk and Humphries opened their article Vaccines: a peek beneath the hood with numerous examples of historical mortality based vax-evangelism. The 2023 publication of Vacunación Libre provides various examples of historical mortality based vax-evangelism as preached in Spain before they go on to debunk those messages. And of course in this essay series I began with extensive documentation of historical mortality based vax-evangelism.
Taking this precaution will not of course stop the vaccine apologists from moving the goal posts, but it will make it difficult for them to gaslight anyone who has seen your argument with the position of the goal posts well documented.
So, how do you document the position of the goal posts? Simply provide examples of the vaccinationists making their historical mortality related claims – their Graveyard Gambits, Bait and Switch Preaching, and Lifespan Lectures. When they make these claims they are establishing the goal posts, and they are responsible for the goalposts being where they are – for it is they who put them there.
If you don’t have your own collection of the vaccine evangelists’ preaching for documentation of where the goalposts are and who put them there, help yourself to the collection that I have put together in this essay series (Exhibits A through T in Part 1 and 4, and now Exhibits U through Z in the appendix of part 7).
5. Child mortality reduction, late vaccine introduction, and low vaccine coverage in Italy
For the final section of this final installment of this essay series we will look at one more set of mortality declines juxtaposed with vaccine introduction.
What makes the Italian mortality data especially noteworthy is that not only did Italy introduce pertussis and measles vaccines relatively late, it also did not initially introduce these vaccines as part of the country’s universal mandatory vaccination program. Most parents did not seek out these optional vaccines (as evidenced by a major 1985 survey). As late as the mid 1980s only a small minority of Italian children were receiving the recommended measles and pertussis vaccines.
The data I’m using for these graphs is from data spreadsheets provided by the Italian National Statistics Institute (Istat) in their 2014 press release Child mortality yesterday and today in Italy.
Istat put together a time series of the Italian cause of death data from 1887 till 2011 (for some reason 2004 and 2005 are missing in their spreadsheets, so I’m simply ending the graphs at 2003).
Istat calculated the deaths for a selection of different causes as an annual death rate for under five year olds per thousand live births. This is ideal and gives us an apples to apples measurement across a time period of significant changes in population size and birth rates in Italy.
Let’s start with whooping cough.
Whooping Cough Mortality in Italy 1887 – 2003
Figure 61
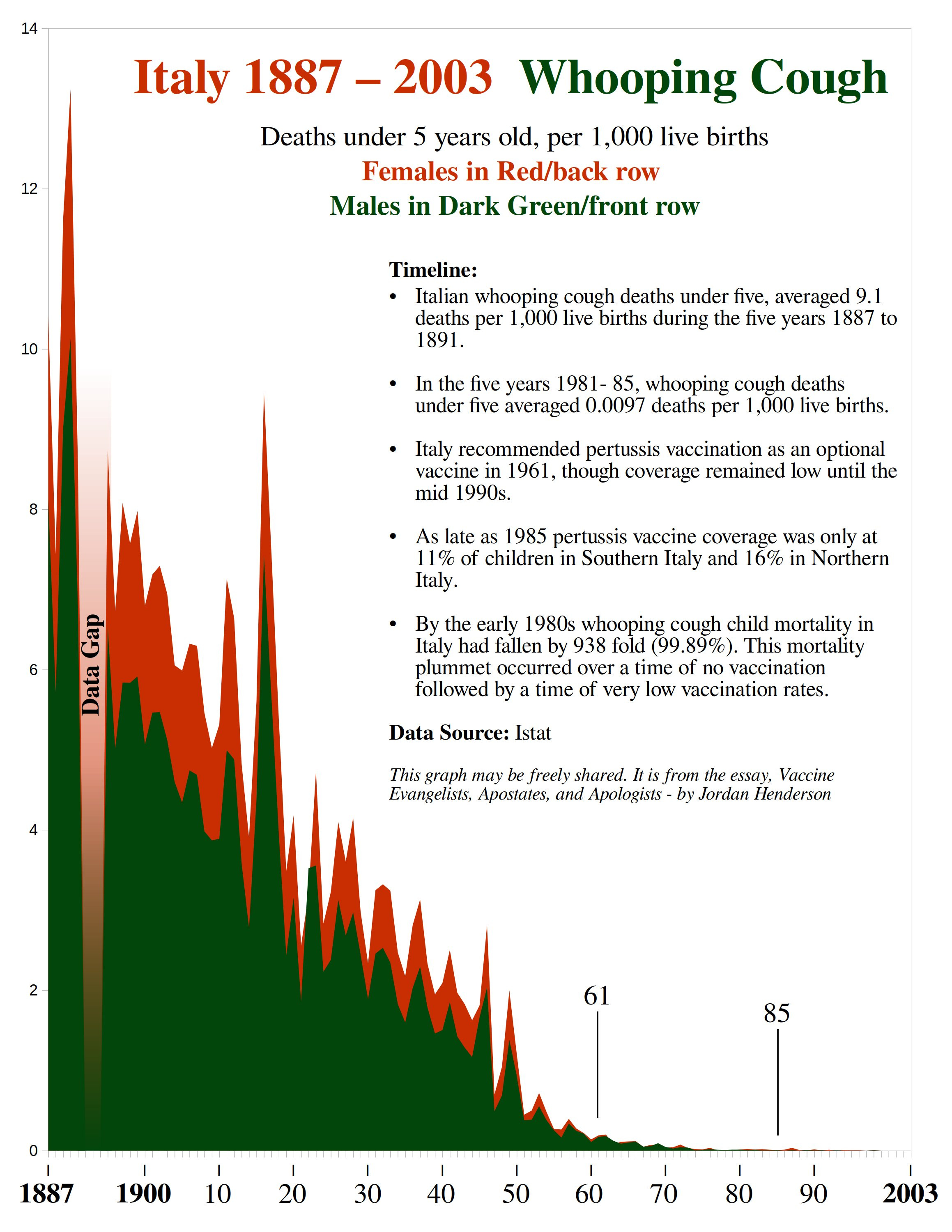
Like everywhere else with old data and late vaccine introduction, we can see that almost all the whooping cough mortality decline happened before Italy’s relatively late introduction of pertussis vaccines in 1961.
Unlike other vaccines in Italy, the pertussis vaccine was not compulsory. In 1985 a large survey was carried out by the Italian Government across multiple regions of Italy to see how many parents were getting their children vaccinated with the optional vaccines, and the answer was . . . not many.
In 1985 pertussis vaccine coverage was only at 11% of children in Southern Italy, and 16% in Northern Italy.
By the early 1980s whooping cough child mortality had fallen over 900 fold or 99.89% from what it had been less than a century earlier in Italy, and again, that is with most Italian children still being unvaccinated against whooping cough.
Now let’s look at measles.
Measles Mortality in Italy 1887 – 2003
Figure 62
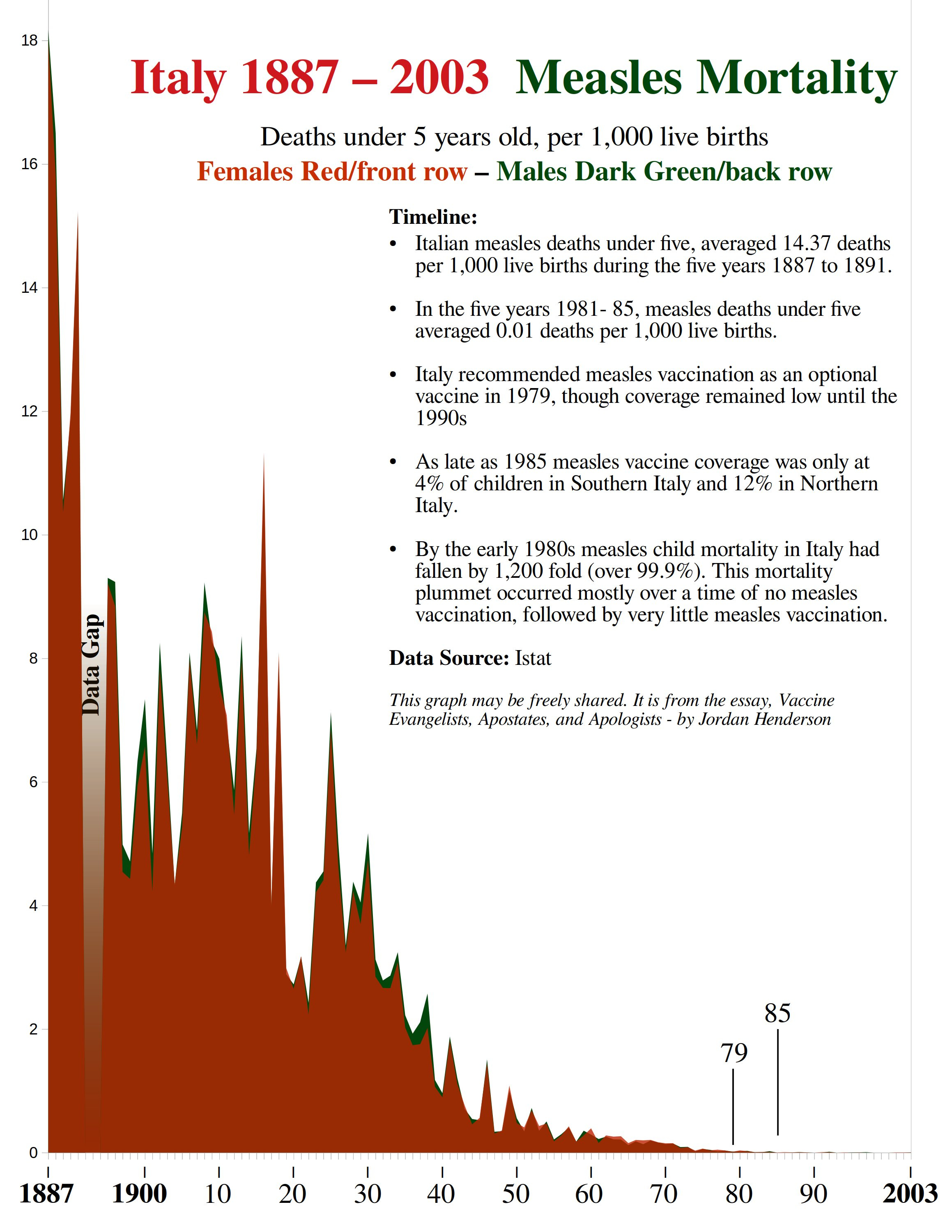
Spain’s greater than 400 fold decline in measles mortality before widespread vaccination was impressive. Belgium’s 544 fold decline is even more impressive, and Sweden looked like it would be the most noteworthy case for measles at just shy of a 1,000 fold measles mortality decline before widespread vaccination.
But here we can see that, at least so far, the title for most impressive measles mortality decline before widespread measles vaccination goes to Italy with a measles mortality decline of 1,200 fold by the early 1980s.
The measles vaccine became commercially available in Italy in 1976. It was officially recommended in 1979. But as with pertussis vaccination, it was not included among the compulsory vaccines, and the 1985 survey to assess uptake of these vaccines found that measles vaccination rates were even lower than pertussis vaccination rates – the 1985 survey found a mere 4% of children had received the measles vaccine in Southern Italy and 12% in Northern Italy.
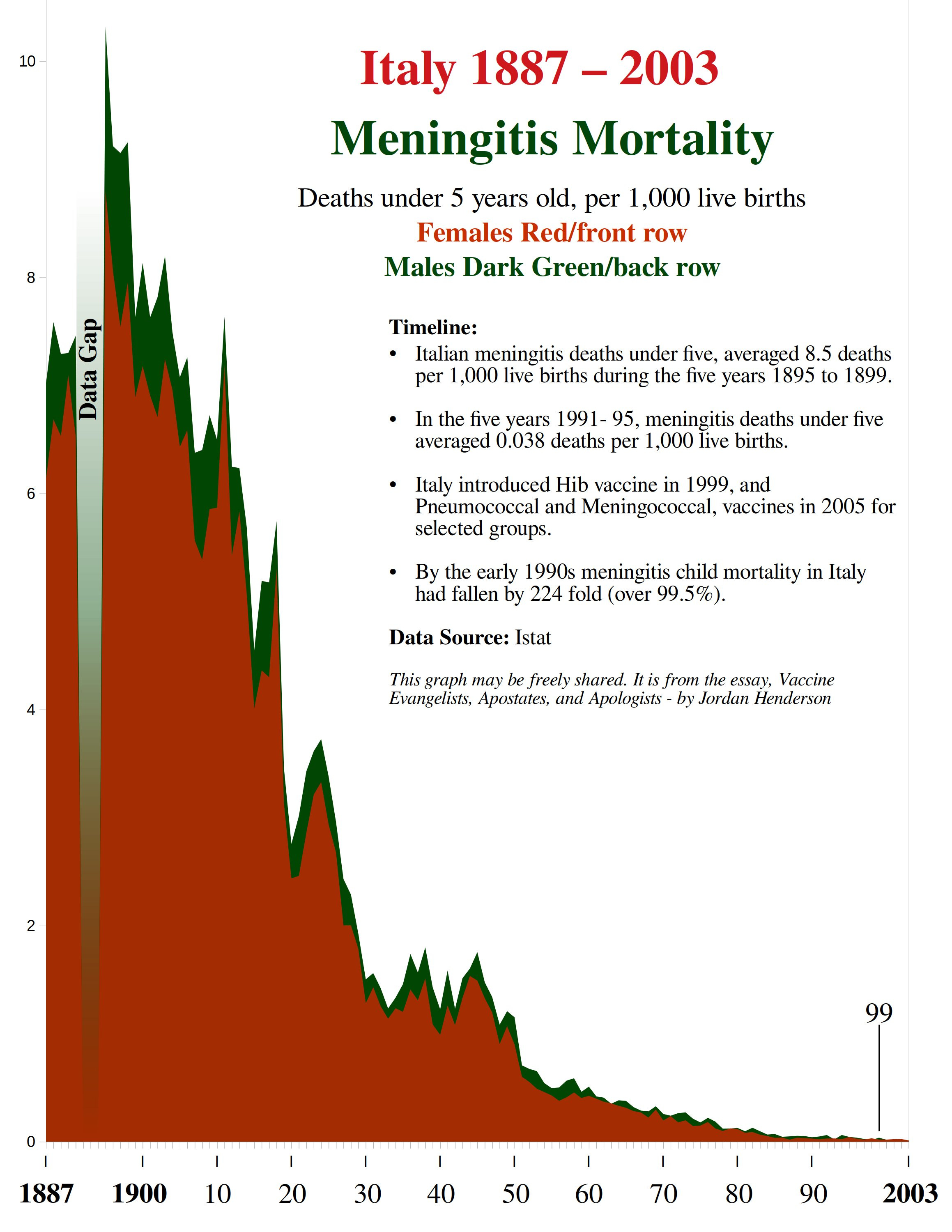
Meningitis Mortality in Italy 1887 – 2003
Here we have another major mortality decline in Italy, with almost all of the decline occurring before relevant vaccines (such as Hib, Pneumococcal and Meningococcal vaccines) had been added to the schedule.
Figure 63
6. Summary
This essay series began with the charge that vaccinationists are and long have been promoting vaccination with powerful historical mortality based messages that are so unhinged from reality that even their own apologists generally avoid directly defending them. I added the additional charge that the apologists were guilty of gaslighting, using a Motte and Bailey doctrine, and general bad faith, because they did whatever they could to avoid acknowledging that their fellow vaccinationists heavily promote these messages to begin with.
I believe that I have provided the necessary and sufficient evidence to prove my case.
The evidence consisted both of a review of other author’s work (primarily Bystrianyk and Humphries, and Greg Beattie) and three original collections of supporting evidence that I provided in this series. These three collections are:
Evangelism - 26 Exhibits of Vaccine Evangelism (Exhibits A through L in Part 1, Exhibits M through T in Part 4, and Exhibits U through Z below in the appendix).
Apostasy – 50+ New graphs of historical mortality from various causes, in different countries and cities, juxtaposed with vaccine introduction. (Found throughout the essay installments and gathered all in one place in the Gallery of Graphs page – More on that below in the appendix).
Apologetics -15 Case Examples of Vaccine Apologetics (Case Example 1 in Part 3, Case Example 2 in Part 5, and Case Examples 3 through 15 in Part 6).
As well as supporting evidence for my arguments, these collections of evangelism, apostasy, and apologetics are meant to be a reference and resource for whoever needs them. Help yourself to the material in those collections as needed.
So ends this 7 Part essay. Below are some more helpful resources in the appendix.
Jordan Henderson lives in Washington State in the Northwest of the United States. He works in oil paints, and charcoals. A portfolio of his works can be viewed at either of his websites: Original Paintings – Fine Art Prints
Appendix: Further Reading & Resources
This essay series has been hyper focused on historical mortality related vaccine questions.
Of course this focus means that I have left everything else to the side. I haven’t touched vaccine risks in this series. I’ve brought up vaccine efficacy only to distinguish it from historical mortality claims. And I intentionally refrained from offering explanations and opinion on what did cause the mortality decline, as it is not strictly necessary for debunking the pro-vaccine historical mortality messages.
All these other areas are of great importance too; their exclusion was purely to keep this essay series focused and within a manageable scope. But now that this series is at its end, it would be good to take stock of major areas of the debate that fall outside this essay’s scope - what we haven’t been looking at.
Smallpox and polio I mentioned in Part 2 of this series as topics that I would be leaving out as they deserve to be discussed at length on their own. I left a selection of recommended reading regarding smallpox and polio at the end of Part 2.
What did cause the pre-vaccine decline is a topic that I may eventually address with an essay on it specifically. In the meantime I encourage readers to share their views and recommended reading on the pre-vaccine mortality declines in the comments.
Suggested reading on the philosophical side of the vaccine debate
Modern Medicine: The Hidden Influence of Beliefs and Fears - Olivier Clerc (brought to my attention by a commentator on a previous article of mine).
Conscience and Vaccines by father Ambrose – Essay here – video adaptation by Dr. Sam Bailey here.
My main contribution, to date, to the philosophical side of the vaccine debate is the essay Science! Blessed be Thy Name: The Vanishing Value of Religious Freedom.
Vaccine Risks
This is another major area of the vaccine debate. Most people probably think that vaccine risks make up the whole vaccine debate. While vaccine risks are only one aspect of the vaccine debate they certainly are an important topic. Here is some recommended reading if you’re looking for suggestions (And do please place your own suggestions in the comments):
The books Dissolving Illusions (Bystrianyk and Humphries) and Vaccination: a parent’s dilemma (Greg Beattie) discuss vaccine risks, as well as a strong focus on historical mortality matters.
Forrest Marready’s book, The Autism Vaccine, centers on the history, development, and dangers, of various diphtheria vaccines and serums.
The book Turtles All the Way Down comprises a tour de force of the scandalous methodology used in vaccine studies to get the “right” answers and avoid inconvenient discoveries concerning vaccine risks.
Pharmaceutical Fraud and the Discovery of Rotavirus – Video by Dr. Sam Bailey
A list of Vaccinated vs Unvaccinated literature from Children’s Health Defense.
Rethinking Disease Paradigms
This is a hot topic that you may have heard as the Virus vs No Virus debate or the Terrain Model vs Germ Theory or something along those lines. Covid-19 placed the Terrain Model vs Germ Theory debate on the radar of most in the Covid-19 opposition. Each side has its enthusiastic supporters and detractors.
The debate of course isn’t new and had been resurfacing well before Covid, especially among AIDS heretics.
The topic is divisive, but feuds and strategic disagreements between different factions of the Covid opposition aside, it is fundamentally a good sign to see so many people re-investigating the foundations of what we have been taught about disease. Renewed interest in rethinking disease paradigms is one of the most promising aspects of the silver lining from Covid-19 in my view.
If you haven’t explored the thinking of the virus skeptics I would encourage you to hear them out.
some good places to start exploring the topic would be the Bailey’s book The final Pandemic, and their video Germ Theory vs Terrain Theory, Mike Stone’s article ViroLIEgy 101: Koch's Postulates, and Boostershots humorous compendium Virus "Denialism" for Beginners.
Gallery of Graphs
For easy reference I have compiled all the graphs that I created for this essay series of historical mortality juxtaposed with vaccine introduction, on a single page. On that page I have also placed many more graphs that I created but did not include in this series due to space considerations.
Expanding the anti-vaccinationist graphical analysis of historical mortality data into many more countries and cities was one of my major goals with this series. You can access the collection on the Gallery of Graphs Page. All those graphs may be freely shared in articles and blog posts, no additional permissions from me needed.
Vaccine Evangelism Exhibits U Through Z
For the reasons I laid out in Section 4 of this Essay ~ Important Strategic Consideration ~ I believe that compendiums of vaccine evangelism are nearly as important a resource in the vaccine debate as compendiums of historical mortality graphs.
The mortality graphs do the heavy lifting in debunking pro-vaccine historical mortality propaganda, but if we don’t first document the goal posts, we leave the Vax-Apologists an easy out. This is where compendiums of Vax-Evangelism come in handy.
Within this essay series there is such a compendium of vaccine evangelism already: I provided 12 Exhibits (Exhibits A through L) of vaccine evangelism in Part 1, along with eight more such exhibits (M through T) in Part 4.
We are only six exhibits away from rounding out the alphabet and including in this series a full 26 examples of vaccine evangelism spanning Exhibits A through Z, so here are six more examples of vaccine evangelism to bring us up to Exhibit Z.
The first two vaccine evangelism exhibits below are examples of what I call the Child Mortality Moralism (Exhibits Q,R, and S from Part 4 also fall under this category). The last four vaccine evangelism exhibits below are Graveyard Gambits. This essay series began with an exhibition of Graveyard Gambits. I think it fitting that we end with them.
~
Vaccine Evangelism Exhibit U
Taxonomic Category – Child Mortality Moralism
The Guardian’s 2021 article No concept of how awful it was’: the forgotten world of pre-vaccine childhood in Australia uses historical child mortality to illustrate the world before vaccines:
“In the 19th century, the leading cause of death in children was infectious disease. People would have 10 children and might lose five of them. We lived with high rates of infant mortality,”
~
Vaccine Evangelism Exhibit V
Taxonomic Category – Child Mortality Moralism
“Infants and young children were and remain the target population for the majority of vaccines due to the high risk of morbidity and mortality in this population. Infectious diseases, including the now vaccine-preventable diarrheal diseases, diphtheria, measles, pertussis, and influenza, were the leading causes of death in US children at the beginning of the 20th century. However, from 1900 to 1998, with the advent of widespread, universal infant and childhood vaccination programs, the proportion of US pediatric mortality due to infectious disease decreased from 61.6% to 2%.”
From the 2012 paper Lessons learned and applied: What the 20th century vaccine experience can teach us about vaccines in the 21st century
published in Human Vaccines and Immunotherapeutics
~
Vaccine Evangelism Exhibit W
Taxonomic Category – Graveyard Gambit
“Historically, many children died before their fifth birthdays (take a look at any historical cemetery and you will see this many tombstones of infants, toddlers, and young children) and this continues today in many third world countries. Since the advent of vaccines and vaccination programs, the numbers have decreased due to the creation of now preventable diseases like tetanus, polio, measles, etc. Vaccines contain the same antigens (or parts of them) that cause diseases, so it prepares your body to one day fight off the actual antigen when exposed by helping it create antibodies now.” (sic)
~
Vaccine Evangelism Exhibit X
Taxonomic Category – Graveyard Gambit
“The Bloomfield memorial and many more like it at Oakland and other older cemeteries illustrate the tragic deaths of children (and adults) from acute infectious diseases in the 19th and early 20th centuries when vaccines to combat these scourges had not yet been developed.
Nearly 30% of the interments at Oakland - which was established in 1850 - are children. Many died from diphtheria, typhoid fever, tetanus, pertussis (whooping cough) and other acute illnesses. These graves are a heartbreaking testament to the fragility of life in that era.
Today, American children and many across the industrial world have little to fear from these dreaded diseases due to the wide availability of the DPT (Diphtheria-Pertussis-Tetanus] and the MMR (Measles-Mumps-Rubella) vaccines that are mandated for all children before entering public school”
“Sadly, there are many among us who eschew the extraordinary value, safety and efficacy of vaccines in providing safe and healthy communities. Now, there are even some political figures who are actually calling for the repeal of all vaccine mandates. Do these people actually want to go back a century in time to when so many died from what are now treatable diseases?”
Excerpts from the 2021 article Visit to historic cemetery shows power of vaccinations published in The Atlanta Journal Constitution.
~
Vaccine Evangelism Exhibit Y
Taxonomic Category – Graveyard Gambit
“Dr. Phyllis Townsend, a pediatrician in Franklin, TN, is concerned about recent trends that leave children unprotected from potentially deadly diseases. “If you walk through an old cemetery, you can see why vaccines are important. Many people lost a child, often under the age of one, from diseases that are completely preventable now,” shares Dr. Townsend.”
From — Dr. Phyllis Townsend Shares How Vaccines Save Lives, a page in the resources and education section of the website of Pediatrics Association of Franklin (Tennessee).
~
Vaccine Evangelism Exhibit Z
Taxonomic Category – Graveyard Gambit
This excerpt (below) is from an ABC News interview with Dr. Lolita McDavid, published in the 2016 article Why Parents Aren't Vaccinating Their Kids, According to New Study
“To help inform parents about the importance of vaccination, McDavid said she gives parents an assignment to go on a field trip to a graveyard.
“I want you to go to an old cemetery, walk through, look at the headstones of the babies that died at age 1, 2, 3 years of age," she said, but thanks to vaccines, "people don’t see this anymore, so people don’t know what to be afraid of.” ”
Thanks for yet another thorough, clear and cogent essay.
You've really done a great job of showing that what vaccinationists lack in intelligence, logic and skill, they clearly make up for in brazen dishonesty.
If deconstructing their transparent bunk is like shooting fish in a barrel, shining a light on Melanie Mallon's spectacular ineptitude is almost embarrassingly so; no wonder you left it out.
Worth repeating: "The vaccine evangelist messages are so far removed from reality that most of the vaccine apologists do not even attempt to defend them and instead spend all their time rerouting conversations, conflating distinct ideas, engaging in shameless projection, gaslighting, and even going so far as to outright deny that their side has been preaching the messages that they are still preaching."
Re: measles ...“They’ve been generating impressive sounding numbers of lives saved by running simulations on models for years.” — Just like the “climate” models … garbage in, garbage out!
I am heartened by the increasing number of people I am meeting who are anti-jab and anti-vaxx, but there are still so many who continue to run around in masks.