


The Red Herring: A Tour of the Motte
Part 3 of Vaccine Evangelists, Apostates, and Apologists

This is the third installment of this essay series. You can read Part 1. The Evangelists at this link here, and Part 2. Apostasy at this link here.
I ended Part 2 with the following description for what’s in store in this essay - Part 3. Here’s how we ended the last essay.
“In the imagery of the Motte and Bailey analogy, the desirable Bailey has been stormed: the Vaccine Apostates knocked over the flimsy palisade, pushed aside a drunken guard or two and took the Bailey.
The Vaccine Apostates accomplished this, as we just saw, by showing us the death data, thereby debunking the belief promoted by the Vaccine Evangelists.
So at this point the Vaccine Apologists lead the retreat into their stronghold, the Motte (comprised primarily of notifications of incidence data), pretend that the Evangelists had never been preaching out in the Bailey to begin with, and accuse the Apostates of attacking a strawman for having stormed the Bailey where their colleagues, the evangelists, had just been preaching.
For Part 3. we’ll focus on notification of incidence data, so that we are familiar with the vaccinationist’s stronghold, and how they use it as a decoy or red herring to get attention off of the death data.”
Through the lens of the Motte and Bailey analogy; the desirable Bailey is the death data, but the death data doesn’t support the Vaccine Evangelists’ message, so when challenged, the Vaccinationists have to retreat to a less desirable but more defensible position based on notification of incidence data (data of reported incidence of diseases. This type of data is also called variously just notifications, incidence, and morbidity).
Before we take a close look at notification of incidence data and how Vaccine Apologists use it to get attention off the death data, let’s briefly recap where we’ve been (feel free to skip to the end of the recap if the first two essay installments are fresh in your mind):
Part 1. The Evangelists provided:
An overview of the vaccine conflict regarding the undue credit given vaccines.
Analogies by which to understand the dynamic within the conflict (Bait and Switch Confidence Games and Motte and Bailey Doctrines).
Terminology – Mortality, Death, Morbidity, Notification of Incidence
An exhibition of Vaccine Evangelist preaching divided into exhibits of the Graveyard Gambit, Bait and Switch Preaching, and the Lifespan Lecture. All these exhibits demonstrated the belief in, and promotion of, the central misconception of the Doctrine of Salvation Through Vaccination.*
(*The belief that vaccines played a primary role in the drastic reduction of deaths attributed to infectious diseases in general, and many major diseases in particular, that occurred in the late 19th and early 20th centuries; and the corollary belief that, these diseases would return with comparable devastation if we stopped vaccination against them.)
Part 2: Apostasy pointed out that both Vaccine Evangelists and Apostates use historical mortality (death) data to make their case, with the revealing difference that Evangelists tell you about the death data, whereas Apostates show it to you.
Then we reviewed the death data for numerous diseases across the English speaking world to see how the Vaccine Apostates have debunked the Evangelist’s preaching by showing us the death data that the Evangelists only told us about.
~ End of Recap ~
To give you the full experience of the Motte, I want you to get the initial tour from one of the Vaccine Apologists themselves. An excellent case example of Vaccine Apologetics that provides a fairly extensive tour of the Motte is Isabella B’s 2015 article Graphical Proof that Vaccines Work. (The link I provided is to the article published on Medium. For good measure here is another link to the same article as an archive on Archive.is.)
Please consider reading Isabella B’s article in full before reading the rest of this essay. I will be deconstructing Isabella B’s article momentarily, and I do not want to ruin for you the full experience of her skillfully argued and clever article; it would be a shame if you didn’t get to first feel the persuasive power of that type of vaccine apologetics, before seeing it deconstructed.
Did you just get back from reading Isabella B’s article? The first reader of this essay found it a little frustrating that I didn’t seem to be in any hurry to get around to deconstructing Isabella’s article and instead spent so much time reviewing dull notifications of incidence data in this essay.
So I’ll take that as a cue that I had better emphasize how this essay is laid out and why: The first two sections of this essay installment are all about exploring the notification of incidence data and understanding the numerous and major differences between notification of incidence data and death data.
I know that familiarizing ourselves with notification of incidence data, and the differences between it and death data, isn’t exactly glamorous, but it is an important step if we are going to have the necessary knowledge base needed to see straight through the Vaccine Apologists.
The notification of incidence data isn’t just a critical part of Isabella’s article, it is a critical part of nearly all the Vaccine Apologetics aimed at dismissing the death data and graphical evidence based on death data such as the information we reviewed in Part 2 Apostasy; the Vaccine Apologists almost invariably retreat into the notifications of incidence data, it is their Motte.
Let me emphasize; I know notifications of incidence data is dull. In terms of evaluating actual disease prevalence much of this type of data is garbage. In terms of debunking the Vaccine Evangelist’s most grandiose preaching, and dispelling the central misconception of the Doctrine of Salvation Through Vaccination the notification of incidence data is irrelevant. I’m not spending this time looking at this throw away notifications of incidence data because I care about it, and I’m not doing it to be mean and cruel to the reader.
I’m walking the reader through this data because this is were the Vaccine Apologists retreat to, and this is the data they use to get your attention off the exciting, consequential, ever so relevant death data. I believe we need to understand and study our opponent’s rhetorical maneuvers, even if their rhetorical maneuvers are based on something as lame as notifications of incidence data.
Then, in the third through sixth sections of this essay installment, we do the glamorous and exciting work of deconstructing vaccine apologetics with the deconstruction of our first case example: Isabella B’s Graphical Proof that Vaccines Work.
The seventh section sums up this installment.
If you’re eager to skip past the notifications of incident data and jump straight to my deconstruction of Isabella’s article go ahead (I can’t stop you anyways!), but please do consider coming back later and reading the first two sections of this essay installment so that you are familiar with these matters in preparation for the extensive deconstruction of the other Vaccine Apologists beginning at the sixth installment.
Let’s begin as before with a table of contents of this next installment of the essay series so that you can see where we’re going at a glance.
Links to the other essays in this series for easy navigation
Part 3 - The Red Herring: A Tour of the Motte (you are here)
Part 6 - The Apologists Continued
Part 7 - The Apologist’s Playbook
Table of Contents of Part 3
1. Graphs of the Notifications of Incidence Data - Case Example: Measles
United States
England and Wales
Australia
Spain
An Honest Appraisal of the Weakness and Unreliability of Notifications of Incidence Data Straight from a Vaccine Apologist
2. Differences Between Mortality and Morbidity Data Revisited
Difference in Relevance
Difference in Gravity/Severity
Difference in Completeness
Difference in Availability
Difference in Value for Indicating Severity of a Disease
3. Case Example #1 of Vaccine Apologetics – Isabella B’s “Graphical Proof that Vaccines Work”
4. General Criticism of “Graphical Proof that Vaccines Work”
Lack of Documentation of the Positions Being Attacked
Repeatedly Commits Post Hoc Fallacy
5. Point by Point Deconstruction of Isabella B’s “Graphical Proof that Vaccines Work” and Identification of the Rhetorical Maneuvers Employed Therein
The section under “Disease incidence is the correct metric” is misdirection
The section under “Mortality rates do not reflect the true burden of the disease” employs the argument from the data we don’t have
The section under “Numerous factors affect mortality rates” is unclear but contains probable: projection, doubles down on misdirection, has a false premise, and has an improbable and unsubstantiated implied premise
The section under “Mortality rates are not more accurate than morbidity rates” is based on misrepresentation of the opposition’s arguments
Fails to substantiate a strong assertion
6. Critical Review of the Graphs in “Graphical Proof that Vaccines Work”
The Diphtheria Notifications Graph
CDC Diphtheria Deception Revisited
The Whooping Cough Notifications Graph
7. Conclusion: The Motte is a Red Herring
Note: the labeling of graphs, exhibits, and case examples, in this essay series is continuous with each essay picking up where the other left off. We left off last essay at figure 15; here we start with figure 16.
This article was originally published on Activist Post, Winter Oak, Valerie Kochmann and Nevermore
1. Graphs for Notifications of Incidence Data - Case Example: Measles
Some notification of incidence data is favorable to the vaccinationists.
In general, measles notification of incidence data is one of the most favorable historical data sets to the vaccinationists. I will be generous to our vaccinationist friends and use measles notifications of incidence as the case example.
Figure 16
In the graph above (from Dissolving Illusions) we can see measles death (mortality) and notifications of incidence data simultaneously. Note that the notifications data is at 1/35th scale. This allows you you to compare the two trends on the same graph; multiply the morbidity (black line) by 35 to get the morbidity rate per 100,000.
Here we can see why Vaccine Apologists would much rather have the conversation center on the notifications of incidence data: while almost all the decline in mortality occurred before the introduction of the vaccine and therefore cannot be attributed to the vaccine, the same cannot be said for the notifications of incidence which did not decline near as much, so at least in theory the vaccine could have played a primary role in the decline of measles incidence.
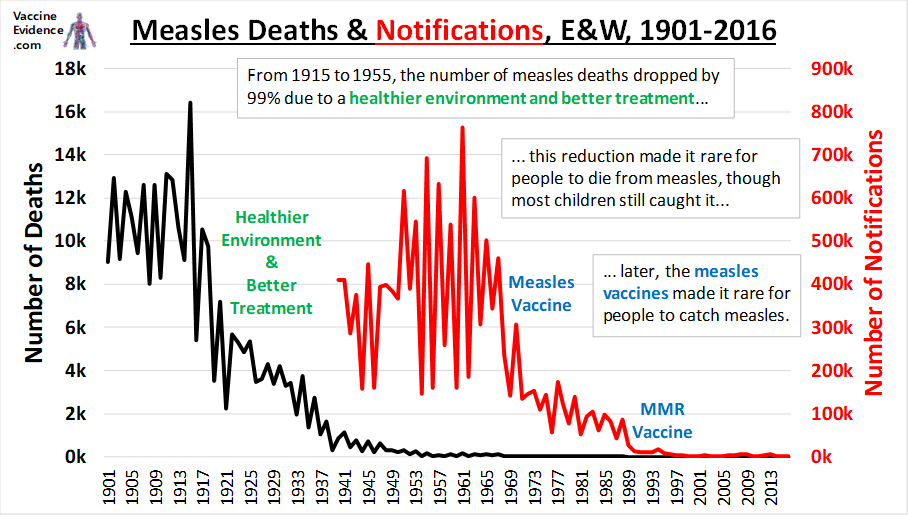
For England and Wales too, the pre-vaccine notifications of incidence remain relatively steady, while the mortality rate plummets.
Figure 17
If we were to take this notifications of incidence data at face value, then the logical implication of measles incidence holding steady while measles mortality plummeted, would be that measles had become a much less dangerous disease and/or children were substantially healthier and measles had become far less of a threat to them. At this link here, on the National Center for Biotechnology Information website (and brought to my attention by this article from VaxInfoStartsHere.com) we can read pages from the British Medical Journal of February 7th 1959 and see, beginning on page 380 of the journal, various first hand physicians’ accounts of their dealings with recent measles outbreaks. These descriptions are in line with the logical inference from the data, that measles had become mild compared to earlier years:
“Dr. R. M. McGREGOR (Hawick, Roxburghshire) writes: In Scotland measles is not a notifiable disease except in the case of certain ports. Information concerning incidence, therefore, is known only to the family doctor and to a lesser extent the school authorities. In this area since 1948 serious outbreaks have occurred in the autumn of 1950, in March and April of 1953, and in June and July of 1955. In the intervening periods, and since the last serious outbreak, sporadic cases have occurred without causing an epidemic. At present we enjoy a complete freedom from this disease, and it is hoped that the act of writing on the subject will not incur the penalty of a visitation.
Scanning the notes of the previous epidemics, it is evident that the 1955 episode was one of low virulence. Indeed, many of the cases were sufficiently mild as to make diagnosis difficult. The follow-up of all the epidemics reveals that the patients have not suffered any permanent disabilities. This could be due to the treatment given being satisfactory or to the excellent recuperative powers of a sturdy population.”
As you can see from the quote above measles wasn’t even a notifiable disease in Scotland at the time, and that’s not uncommon for notifications of incidence data to be missing entirely for many diseases in many places. Case in point, let’s look at measles notifications of incidence data, or lack thereof, in Australia from Greg Beattie’s book Fooling ourselves on the fundamental value of vaccines.
Figure 18

Here is an excerpt of Beattie’s commentary about this:
“In the case of measles, we immediately see that 40 years of data is missing surrounding the introduction of the vaccine. Notifications were not compiled nationally from 1949 to the mid-1980s when the National Campaign Against Measles began. Even the data prior to 1949 is scanty. Measles was not a notifiable illness in most states.” - Greg Beattie: Fooling ourselves on the fundamental value of vaccines.
An Honest Appraisal of the Weakness and Unreliability of Notifications of Incidence Data Straight from a Vaccine Apologist
Let me show you how we can get an honest opinion from the vaccinationists themselves about notifications of incidence data:
If a morbidity data set shows what the vaccinationists want to see, they of course are happy to take it at face value, but all it takes to get the vaccinationists to speak plainly about the unreliability of the notifications of incidence data, is a morbidity data set that they are none to happy about, like this one:
Figure 19
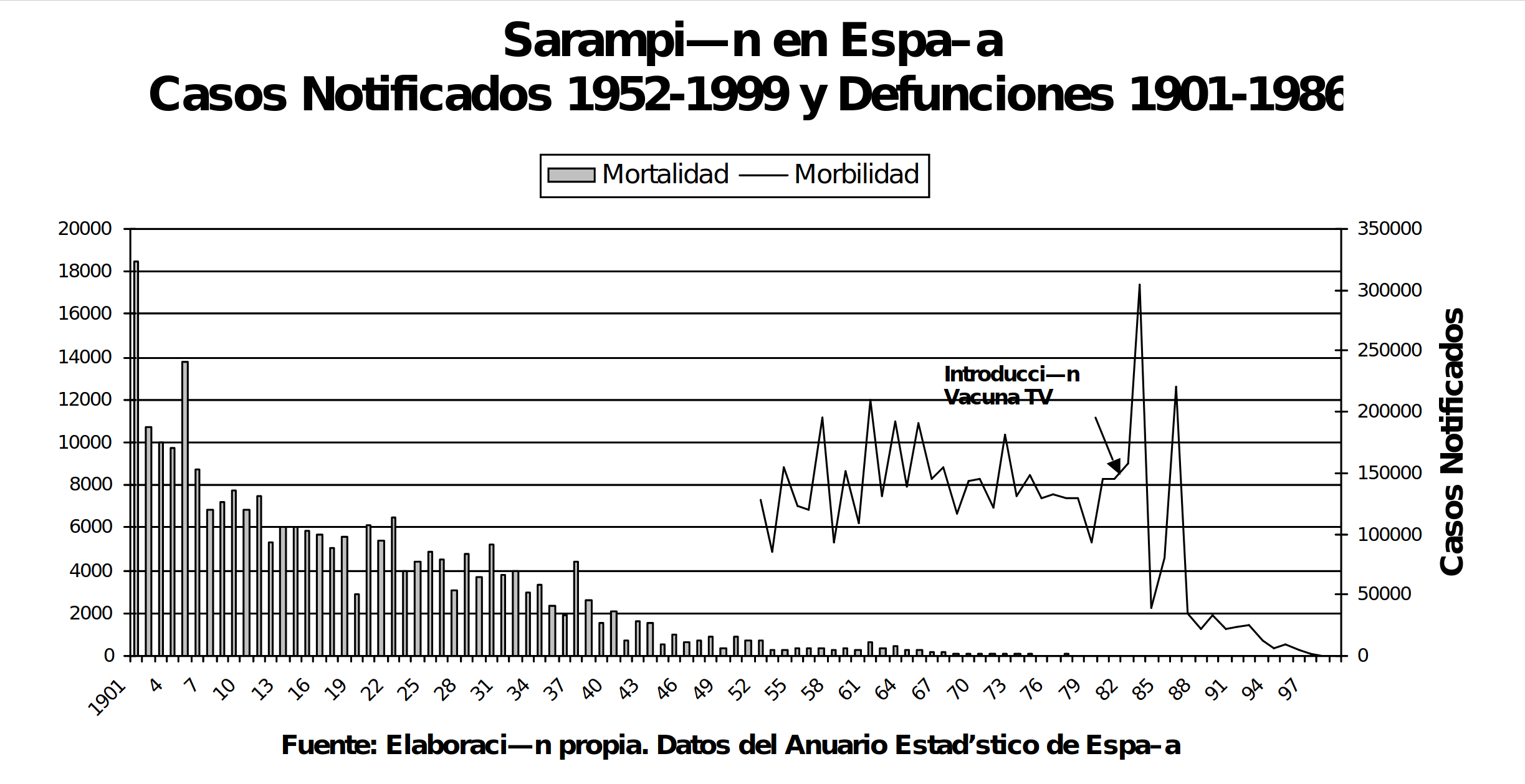
Figure 19 is a screenshot from this document from the Spanish website VacunacionLibre.org. This graph juxtaposes mortality and morbidity data for measles (sarampión) in Spain. The bar graph is the death data and the line graph is the notifications of incidence data. The measles vaccine program was introduced in Spain beginning in 1978,* and the MMR Vaccine in 1981 (MMR vaccine in Spanish is Triple Vírica [triple virus] = TV for short, as seen in figure 19). The data source is the Statistical Year Books of Spain (Anuarios Estadísticos).
(*An earlier measles vaccine pilot program was implemented in Spain in 1968 but was suspended in 1970 due to high levels of adverse vaccine reactions.)
Here we can see that for Spain also, almost all the reduction in measles deaths occurred before the introduction of the measles vaccine. Here too we see that notifications of incidence for measles in Spain hold relatively steady and do not plummet as does mortality. In fact, notifications of measles incidence data reached all time highs in Spain after measles deaths had reached all time lows. The two data sets diverge, one from the other, almost completely.
The vaccinationists will of course credit any decline after the introduction of the vaccine, to the vaccine, but the notifications of incidence data for Spain does pose a problem for the vaccinationists:
The highest number, by far, of measles notifications of incidence for Spain happens in the year 1983, six years after the introduction of measles vaccines in Spain. The second highest year for measles notifications in Spain is the year 1986 by which point right around 400,000 thousand doses of measles vaccine were being given each year, and that in a nation where live births had dropped to around 450,000 a year.
(You can verify these numbers in the Statistical Yearbooks of Spain or more easily in this document here from the Carlos III Health Institute – No worries if you don’t read Spanish as I can walk you to the relevant pages and save you some time with the following instructions. Besides it’s mostly numbers, just remember that they use the period like we use a comma when writing numbers:
Yearly number of live births on page 35 [under the column - natalidad] of the Carlos III document.
Measles notifications of incidence on page 191.
Measles vaccine doses administered per year on page 238. Remember to add the columns for both sarampión/measles vaccination by itself, and the column for measles with mumps and rubella, the “Triple V” [MMR] to get the total measles vaccine dosage per year.)
Compare the Spanish mortality and morbidity data (above in Figure 19 of this essay) to the US mortality and morbidity data (Figure 16). Vaccinationists claim that the plummet in the notifications of incidence data in the US is due to the measles vaccine, even though the measles vaccination rate in the US was only around 60% in the first years of MMR in the late 1960s (I haven’t found documentation of measles vaccine coverage before MMR).
Then in Spain we see not only the two highest ever years for measles notifications of incidence well after the introduction of measles vaccines, we see that the second of these two worst years for measles notifications of incidence comes after measles vaccinations have reached around 8 doses per 9 children born*; a higher vaccination rate than the vaccination rate in the US which allegedly caused the plummet in notifications of incidence in the US.
*(the measles vaccine is generally given at 12 to 15 months, and 9 months during the beginning of the vaccination program in Spain, so the number of children born one year gives us the approximate number of children the following year for whom the vaccine is recommended. Initially the Spanish vaccine program would have had catching up to do for the unvaccinated children under 11 born in previous years, but by 1986 the program had already been in place for nine years)
Let us be consistent: if we credit the low measles notifications numbers following vaccination as directly attributable to the vaccine in the US, then why don’t we also attribute the worst years ever for notifications of incidence following the vaccine in Spain as directly attributable to the measles vaccine?
Clearly the vaccinationists would not be okay with that, so how then do Spanish Vaccine Apologists deal with the Spanish measles notifications of incidence data?
In the paperback, 2018, third printing of the book EN DEFENSA DE LAS VACUNAS (In Defense of Vaccines) by the Spanish pediatrician and Vaccine Apologist – Carlos González, we find several pages, from page 179 to page 184 dedicated to faulting Spanish Vaccine Apostates for pointing out that the highest ever numbers of notifications of incidence occurred well after the initiation of the Spanish measles vaccine program.
González explains, on page 183:
“The declared cases of measles, during the time in which it (measles) was very common, were always underestimated: when a doctor sees dozens of cases, it is easy to forget to declare a good part of them. When vaccination was introduced the issue would have been discussed. The doctors were sure to receive information about measles and its importance, and they talked about it in the press and even on TV. Doctors probably took more care in reporting the measles cases they saw. Therefore, the incidence figures after the start of vaccination probably remained undervalued, but are closer to reality than the previous ones. That is, the peak we see in the graph is because yes, there was an epidemic of measles, but also that they (the doctors) put more care into trying to declare all cases.”
And here is the original Spanish for those who would like to double check it lest anyone accuse me of translating unfavorably.
“Las cifras declaradas del sarampión, en la época en que era muy frequente, estaban siempre infravaloradas: cuando un médico ve docenas de casos, es fácil que se olvide de declarar una buena parte. Cuando se introdujo la vacunación debió de hablarse del tema. Seguro que los médicos recibieron información sobre el sarampión y su importancia, y se habló en la prensa y hasta en la tele. Probablemente los médicos pusieron más cuidado en declarar los casos de sarampión que veían. Por lo tanto, las cifras de incidencia tras el inicio de la vacunación probablemente siguen estando infravaloradas, pero son más próximas a la realidad que las anteriores. Es decir, el pico que vemos en la gráfica se debe a que sí, hubo una epidemia de sarampión, pero también a que se puso más cuidado en intentar declarar todos los casos.”
And that is how Spanish Vaccine Apologists deal with those inconvenient spikes in measles after the vaccine program started: they simply point to the unreliability of notifications of incidence data, and note that you can’t take it at face value; according to González the highest years ever for measles notifications of incidence in Spain, may really not have been any higher than previous years, and could simply be attributable to measles being hyped more during those years.
That’s what I mean; to get a frank admission of the weakness and unreliability of the notifications of incidence data from the vaccinationists, just listen to them explain away a notifications of incidence data set that shows something they don’t like.
2. Differences Between Mortality and Morbidity Data Revisited
In Part 1, of this essay series we went over the terminology of Mortality, Death, Morbidity, and Notifications of Incidence. I emphasized keeping the differences between them in mind; let’s expand on that:
Difference in Relevance
Mortality data is the relevant data source for evaluating and placing in context the central misconception of The Doctrine of Salvation Through Vaccination:
The belief that vaccines played a primary role in causing the drastic decline in deaths attributed to infectious disease in general, and many major diseases in particular, that occurred in the late 19th and early 20th centuries, especially as this relates to the plummet in infant and child mortality rates; and also the corollary belief that, these diseases would return with comparable devastation if we stopped vaccination against them.
One dozen case examples of Vaccine Evangelists promoting this misconception were provided in the first installment of this essay series, Part 1: The Evangelists, in Exhibits A through L.
The preaching of the Vaccine Evangelists such as the Graveyard Gambit, the Bait and Switch Preaching, and the Lifespan Lecture, cannot be verified, nor falsified, nor placed into context through notifications of incidence data, but it can be through mortality data. Because they are preaching about lives saved through vaccination, and the number of lives lost to infectious diseases before vaccination, they need the death data to support the belief that they are promoting.
As I wrote in Part 1: The Evangelists:
Morbidity data would be icing on the cake of that belief, but the belief is indefensible to begin with if the mortality data doesn’t support it (in which case there is no cake to put the icing on).
Difference in Gravity/Severity
This is quite straightforward, and needs no further elucidation, so I’ll just quote myself from Part 1 as a refresher for the reader.
Experiencing an illness (morbidity), which might be very mild, and may not result in any lasting complications, is very different from experiencing death (mortality) which means the end of your earthly visit, and the defunction of all the bodily functions of your physical body. There is no “mild death.”
Morbidity might lead to mortality or it might not even remotely head that way; these are two potentially and often radically different conditions. Morbidity could refer to just about any condition, including something very temporary, that results in something just shy of excellent health, but is still a literal lifetime away from death.
Difference in Completeness
Many of the historical, death by cause of death, data sets, are mostly complete data sources, in that most the deaths were recorded for the areas represented in many of the data sets:
Here is an example; the 1920 Mortality Statistics of the United States by the Bureau of the Census specifies on page 10 that states and cities had to have nearly complete death registration, recording at least 90% of deaths in order to be included in the United States death registration area. That's not to say that they actually did successfully achieve 90% registration of deaths, we probably won’t know for sure, and their methods for gauging completeness may have been faulty, but it is evidence that death registration data was held to standards that notifications data was and is not. At least some demonstration of completeness was required for the death data to be considered worthy of inclusion in the yearly statistics.
Some places achieved nearly complete death registration sorted by cause even in the 19th century; For example: Massachusetts as early as the 1850s is regarded as having had excellent registration of deaths. This paper, THE ACCURACY OF VITAL STATISTICS IN MASSACHUSETTS, 1842-1901 Gutman, Robert estimates that in 1855 Massachusetts was only failing to record 11% of deaths, which works out to 89% complete death registration, and on page three Gutman notes:
“by 1870, registration of deaths had become virtually complete” (for Massachusetts)
Notification of incidence data by comparison is very much incomplete: the CDC’s measles page, states that, prior to the vaccination program half a million measles cases were reported each year, but they also estimate that 3 to 4 million people actually got measles each year.
Using the CDC’s own estimation of the actual number of measles incidence (3 to 4 million) vs the reported number of measles cases (½ a million) we can see that only 1 out of 6, or 1 out of 8 incidences of measles were actually being reported.
For Spain also, the morbidity data is very much incomplete; González stresses how under reported incidence was multiple times. On page 182 of his book (En defensa de las vacunas, 2018 paperback third printing), he notes that while rare, grave diseases such as yellow fever, are well reported, mild cases of illnesses such as the flu and measles are not well reported. His own words are that:
“The official numbers are very underestimated, and only serve to show if tendency/prevalence, increases or decreases from one year to another.”
(And as before, here is the original Spanish to demonstrate that I translated fairly.
“Las cifras oficiales están muy infravaloradas, y solo sirven para ver la tendencia, si aumentó o disminuyó de un año a otro.”)
And as we saw, González regards the incidence notification data as not even necessarily accurate for the purpose of gauging year to year trends, for he noted that the record high years for notifications of incidence following measles vaccination in Spain may simply be because of increased news coverage, and messaging sent to doctors.
We should take note, though, that Gonzalez believes grave diseases are relatively well reported. In the US literature, we also find it noted that while “diseases such as measles are poorly reported,” diseases considered very serious do tend to be well reported, or at least that’s what the official documents claim (emphasis mine):
“The completeness of reporting communicable diseases varies from State to State and in different parts of the same State. Several variables influence the reporting of diseases. Certain so-called minor communicable diseases such as measles are poorly reported because a large proportion of the cases are never seen by a physician. The fact that few cases of measles have a fatal termination and because restrictive measures are minimum and no investigation of cases is made, also mitigates against complete reporting. On the other hand, a very high proportion of the potentially dangerous diseases such as smallpox, diphtheria,* and typhoid fever, are reported.”
Vital Statistics of the United States – 1950 Page 63, Chapter 4, Notifiable Disease Statistics.
[*Relevant to revisiting the CDC’s diphtheria deception at the end of this essay]
Isabella B, whose work of vaccine apologetics we are about to critically review as a case example, also notes the very much incomplete nature of notifications of incidence data in Graphical Proof that Vaccines Work. Regarding notifications of measles incidence in England, Isabella B writes (emphasis in the original);
“In the pre-vaccination period, when measles infection was universal, the number of actual cases would have been much higher than the number of reported cases, as only a fraction were reported to the public health care system during that time.”
The Vaccine Apostates, of course, are keenly aware of these differences in the data types; for example Greg Beattie in his book Fooling ourselves on the fundamental value of vaccines devotes multiple, very informative chapters, to a discussion of notifications of incidence data, and its shortcomings.
We can see that completeness is yet another major difference between the morbidity and mortality data, and the vaccinationists also acknowledge this (i.e Isabella B and Carlos González above) even if they have a disturbing tendency to conveniently forget this difference most the time.
Difference in Availability
A notable quality of the notification of incidence data is that much of it is missing, because it was never collected to begin with for many of the most interesting and crucial times:
For England and Wales we find the notification of incidence data for many of the diseases only gets us back to the 1940s, leaving us without corresponding notifications data for the period in which most the decline in mortality occurred. The mortality data in contrast is available from 1838 onwards.
For most the Spanish data, the notification of incidence data is not available nationally till the mid 1940s, leaving us without national notifications for the period in which most the 20th century decline in mortality occurred. By contrast death/mortality data sorted by cause is available for Spain back to 1900.
In the United States national notification of incidence data is not available till:
1912 for diphtheria, measles, typhoid, polio
1922 for whooping cough
1930 for tuberculosis
1912 is only 12 years later than the collection of national (but really - death registration area) yearly cause of death data in the US, but for a disease like diphtheria that’s a lot of missing data; over half the recorded US 20th century decline in diphtheria mortality happened before 1912, leaving us with no corresponding notification of incidence data for the period in which the greatest part of the 20th century plummet in diphtheria mortality occurred.
For Australia they were not consistently making many of these diseases notifiable at all. Figure 18 showed us the enormous amount of missing measles notifications of incidence data for Australia, here is another graph of Australian notifications of incidence data or lack thereof from Greg Beattie’s book Fooling ourselves on the fundamental value of vaccines, this one for whooping cough.
Figure 20

Beattie writes of the Australian whooping cough notifications of incidence data:
“With whooping cough, we see a 30 year gap where data was not compiled nationally. Prior to this, it came predominantly from one state (SA). In fact, examination of the raw data reveals it was not until 1982 in NSW, 1983 in NT, 1989 in Tasmania, and 1990 in Queensland that the illness was even notifiable.”
Availability as we can see, is another major difference between morbidity and mortality data with much of the morbidity data missing altogether.
Difference in Value for Indicating Severity of a Disease
Neither mortality nor morbidity data will show you the number of serious complications other than death attributed to a disease. Historical data sets comparable to mortality data in which nearly all serious disease injuries are listed year by year and sorted according to cause do not exist, or at least no one on either side of the debate knows where to find any such data set. Just in case such a data set is hiding somewhere unknown to nearly everyone, I emailed the CDC twice asking if they knew of any such data; months later I’m still awaiting a response (not that I expect one at this point).
We can, however, get a rough estimate of the serious complications burden of a disease by extrapolating from the data we do have, but only one of the data sets is suitable for that – death data. Prevalence of a disease (of which notifications of incidence data is used as a weak and unreliable gauge) is no indicator of the severity of the disease. Death, by contrast, most certainly is an indicator of severity.
Vaccine Apologists frequently do something that I call arguing from the data we don’t have. This involves downplaying the value of mortality data by pointing out that death is not the only serious outcome that a diseases can cause. They then fault the Vaccine Apostates for not providing historical data on the rate of various serious disease complications other than death, and then they switch the conversation back to notifications of incidence data.
By appealing to the yearly historical data of serious complications other than death for various diseases, sorted by cause, the Vaccine Apologists give the impression that this data would support them if it existed. But they don’t provide this data . . . evidently because they can’t find it.
They will generally give estimates for the number of serious complications per thousand but provide no continuous series of complications data that would allow us to assess the pre-vaccine trend.
The reason Vaccine Apostates are not creating graphs of historical data for various serious complications other than death from different diseases is because, just like the Vaccine Apologists, the Apostates cannot find such data either.
That’s why I call it arguing from the data we don’t have when the Apologists fault the Apostates for not showing graphs of the data that the Apologists can’t find either.
There is, however, one serious disease complication for which do have extensive, historical data sorted by cause – death.
3. Case Example #1 of Vaccine Apologetics - “Graphical Proof that Vaccines Work”
I hope you have had a chance to read Isabella B’s 2015 article Graphical Proof that Vaccines Work (Archive.is Version Here).
Here is some background before we get into the deconstruction of Isabella’s article: I first knew of Isabella B, whoever she may be, when reading critical reviews of the book Dissolving Illusions. I wanted to see how the book, Dissolving Illusions, stood up to criticism.
Some of the most detailed criticism at the time was actually on the Amazon reviews for the book. The most serious and skillfully argued critical review was one Isabella B had written. A lengthy debate ensued right there on the Amazon reviews for the book, between Isabella B and one of the Dissolving Illusions authors, in responses and counter responses to Isabella B’s review.
Isabella B followed this up by moving her criticism of the book out from the reviews section onto the general internet with the 2014 article Why Dr Suzanne Humphries, an anti-vaccine activist, is lying to you about measles, to which Humphries and Bystrianyk responded with Response to “Isabella B’s” “Why Dr Suzanne Humphries, an anti-vaccine activist, is lying to you about measles”
Isabella B then branched out from criticizing Dissolving Illusions into more general Vaccine Apologetics, published several articles in succession, and then apparently moved on and left the topic behind.
I chose Isabella B’s 2015 article Graphical Proof that Vaccines Work to have the honor of being Case Example #1 of Vaccine Apologetics for this essay series because:
Her article provides an excellent tour of the Motte/overview of incident notifications data.
It’s skillfully argued and clever.
It is solidly representative of Vaccine Apologetics aimed at dismissing or downplaying death data; all the Apologists basically use slight variations of the same arguments Isabella B uses to get the attention away from the death data. And few of the Apologists are as skilled at this as is Isabella B.
The continued relevance of Isabella B’s article is evidenced by the fact that it continues to be quoted from and linked to right up into the 2020’s: Here, we see this article quoted Isabella with five excerpts strung together from her article to support the author’s point, Isabella’s article is linked to here in an ourworld in data page that was revised in 2022, or here on the imminization page of the Immunization Foundation of Australia which had to have been updated or created after 2020 based on the content and, and so on, and so forth.
Suffice it say Isabella’s article has had a good run, and the article appears to still be alive and well (see above[4]). It has served the vaccinationists admirably, but it is well past time to put Isabella’s article out to pasture; I will now open the pasture gate and usher it through.
~
4. General Critique of “Graphical Proof that Vaccines Work”
~
Lack of Documentation
Who is Isabella criticizing? She does not tell us, and does not provide documentation of her opponent’s claims. This leaves Isabella free to misrepresent her opponent’s claims by not allowing us to verify whether or not they are saying what she says they are saying.
Isabella does give us a clue, though, as to who she is likely criticizing when she singles out her principal target, or type of target (emphasis in the original):
“Proponents of the anti-vaccine movement will often plot death rates over time”
The death rate graphs that circulate in the English Speaking sphere of the vaccine conflict are primarily by Bystrianyk and Humphries, and by Greg Beattie. Isabella B’s lack of documentation gives us no choice but to decide for ourselves whom she is criticizing; I deem it fair to judge Isabella’s claims against the work of Bystrianyk and Humphries, and Greg Beattie, as the most probable people who Isabella is taking aim at.
Repeatedly Commits Post Hoc Fallacies
Wikipedia gives a pretty good overview of a post hoc fallacy:
“The fallacy lies in a conclusion based solely on the order of events, rather than taking into account other factors potentially responsible for the result that might rule out the connection.”
“A occurred, then B occurred.
Therefore, A caused B.”
"The rooster crows immediately before sunrise; therefore the rooster causes the sun to rise."
Isabella treats a vaccine as having merely come into existence at some point before a decline in death or notifications as reason enough to conclude that the vaccine caused the decline in incidence or mortality from that point on.
The vaccine came into existence, then the notifications rate fell.
Therefore the vaccine caused the fall in notifications.
There is no exploration or acknowledgment in Isabella’s article of other factors that could have caused the respective declines. No consideration is given, nor investigation made, into the most basic areas to look, such as possible changes in disease definition, reporting requirements, diagnostic criteria, or diagnostic bias.
~
5. Point by Point Deconstruction of Isabella B’s “Graphical Proof that Vaccines Work” and Identification of the Rhetorical Maneuvers Employed Therein
~
The section under “Disease incidence is the correct metric” is misdirection
The most important rhetorical maneuver that Isabella makes in her entire article occurs in the first three paragraphs (emphasis in the original):
“The graphs in this article (showing disease incidence over time relating to several diseases and several countries) make a compelling case for vaccine effectiveness.
Proponents of the anti-vaccine movement will often plot death rates over time as “proof” that vaccines were introduced at a time when they had a negligible effect. However, mortality rates are the incorrect metric when evaluating vaccine effectiveness. Here’s why:
Disease incidence is the correct metric. Since vaccines are designed to prevent the incidence of disease, rates of disease (morbidity) are the correct metric for evaluating vaccine effectiveness. If vaccines were a drug to treat disease, then case-fatality rates would be the correct metric for evaluation. Measuring vaccine effectiveness by looking at mortality rates only is a bit like measuring contraceptive effectiveness by measuring abortion rates only — it only tells a tiny part of the story.”
- Isabella B - Graphical Proof that Vaccines Work
That right there was beautifully executed: every Vaccine Apologist has to figure out how to make the switch without alerting the mark; they have to substitute the bait from the Evangelists’ preaching about vaccines adding 30 years to our lifespan, and ending the age of cemeteries filled with little kids headstones, to the switch of “vaccines reduced notifications of incidence.”
They have to retreat from the death data Bailey into the notification of incidence Motte without it looking like they are ceding any ground or running for cover.
How did Isabella pull off that rhetorical maneuver? She employed a very basic technique that can be summed up in the following statement.
This saw is no good because it doesn’t hammer nails.
The saw may be no good for hammering nails, but if what you want to do is saw wood than the saw is appropriate.
Fault a tool if it doesn’t do what it is supposed to do. Don’t fault a tool for not doing what it wasn’t meant for to begin with.
Isabella B is faulting the death rate graphs for not being the appropriate tool for “evaluating vaccine effectiveness.” Her argument against the relevance of the death rate graphs is based on the premise that the principle purpose of these graphs is to evaluate vaccine effectiveness. But this is not the principle purpose of death rate graphs.
While some of the historical death rate graphs can be be used as an indicator of vaccine effectiveness in certain instances, the primary purpose of the death rate graphs is to remove undue credit from vaccines by demonstrating what vaccines did not do.
Whether or not vaccines are effective, and whether not vaccines did what they are claimed to have done, are two separate questions.
Q - What primarily do Vaccine Apostates use death rate graphs for?
A – To remove undue credit from vaccines by demonstrating what vaccines did not do.
Most the death rate graphs we have looked at do not tell you whether or not the vaccines in question work. What these graphs do show you is what the vaccines in question did not do. For example, the US measles death rate graph demonstrates that the measles vaccine did not cause the greater than 98% plummet in the measles death rate that occurred before 1963, because that decline occurred before the vaccine’s introduction.
We have seen that, contrary to all the Vaccine Evangelism we reviewed in the first installment of this essay series (Part 1: The Evangelists Exhibits A through L), vaccines did not add 30 years to our lifespan, vaccines are not the reason we no longer have graveyards regularly peopled by children taken by childhood diseases, and vaccines are not the reason the USA no longer has 9,000 pertussis deaths a year.
The death rate graphs are an effective tool for dispelling such misconceptions and debunking Vaccine Evangelist preaching.
Did Bystrianyk and Humphries call their book “Evaluating Vaccine Effectiveness” ? No, they called it Dissolving Illusions: Disease, Vaccines, and The Forgotten History.
They dissolved illusions about vaccines, by showing through overlooked historical information that vaccines had received undue credit for accomplishments that had been caused by other factors. One of their tools for removing this undue credit from vaccines was death rate graphs showing us what vaccines did not do.
Greg Beattie in turn opens his book Fooling ourselves on the fundamental value of vaccines with a detailed example of Vaccine Evangelists preaching the Graveyard Gambit in which vaccines are credited for the improvement in child mortality from what it was in the 19th Century.
Beattie makes it very clear that he is using the death rate graphs to refute the type of misconception evident in the Graveyard Gambit example that he provided, by demonstrating what vaccines did not do.
Beattie goes on to explicitly state, on page 13 of his book:
“These graphs do not make any attempt whatsoever to measure the performance of a vaccine. They simply put things into historical perspective for us. This perspective illustrates that vaccines were unimportant influences in the bigger picture; that they arrived too late to be considered potential contributors of any significance.
In Chapter Three we will examine (under a microscope) the contribution that vaccines made to the tail end of the declines. For now, let us simply acknowledge that, in historical perspective, vaccination made little if any contribution to the decline in deaths from each illness.”
The Vaccine Apologists cannot acknowledge the principal purpose of these graphs no matter how obvious it is what these graphs are being used for. The reason they can’t acknowledge this is because clearly these graphs are an effective tool for doing what they are intended for. The only way to judge death rate graphs to be irrelevant or inapplicable, is to judge them by their usefulness as a tool for something that is not their primary purpose.
The Vaccine Apostates are using a saw to saw wood. The Apologists have no way to dismiss the appropriateness and effectiveness of the saw other than by faulting the saw for not hammering nails.
With care the Apologists can pull off this sleight of hand sufficiently well to fool unwary readers.
The section under “Mortality rates do not reflect the true burden of the disease” employs the argument from the data we don’t have
The next point Isabella makes is a Vaccine Apologist favorite: the argument from the data we don’t have (emphasis is from the original and is a subheading, also I updated the Oxford Journal link she gave [1] which had since become broken):
“Mortality rates do not reflect the true burden of the disease. Survivors of vaccine preventable disease can be maimed for life — think polio and paralysis, mumps and deafness, measles and mental disability, rubella and birth defects. Looking at mortality rates only misses the true burden of the disease. For example, before the introduction of the measles vaccine in the US in the 1960s, there were “only” 400–700 measles deaths a year. However, there were 4,000 cases of measles encephalitis a year (many of which led to neurological complications such as blindness, deafness and mental disability), 150,000 cases of respiratory complications, and 48,000 measles-related hospitalizations a year (which placed a huge financial and emotional burden on families) [1]. Together, these figures added to the motivation to eradicate the disease.”
- Isabella B - Graphical Proof that Vaccines Work
Isabella B, provides many notifications of incident graphs and a few death rate graphs, but Isabella provides no graphs with serious complications other than death. Why doesn’t she provide such graphs, since she just stressed the importance of serious complications (“think polio and paralysis, mumps and deafness, measles and mental disability, rubella and birth defects”)? Most likely because she can’t find any data sets of yearly, serious complications, sorted by cause. The reason Apostates provide no such data either is because they, too, cannot find such data.
Isabella does provide a yearly estimate of measles encephalitis and hospitalizations, but in order to place this in context we need to know the trend; we need to know if the complications and hospitalizations were holding steady, rising, or plummeting before the vaccine.
To get a picture for disease complications that would be of comparable reliability and worth to the death data, we would need a serious complications data set that was comparably complete, and comparably old.
Isabella B is telling us about this data, but she isn’t showing it to us. To be fair, that’s almost certainly because she cannot find it. But also to be fair she should not fault the Apostates for not showing us the data that she can’t show us either.
Do you remember the examples of Bait and Switch Preaching in the first installment of this series? (Part 1: The Evangelists - Exhibits E, F, G, and H) In every one of those exhibits only statistics for death and notifications of incidence were mentioned by the Vaccine Evangelists; is that because the Vaccine Evangelists don’t care about serious complications other than death? Of course not; the Evangelists mentioned the yearly number of deaths and notifications of incidence because those are the data sets that exist and are available for those time periods.
Isabella B uses a display of concern for serious complications as an excuse to downplay the one serious disease complication for which we actually do have extensive, yearly, mostly complete, sorted-by-cause data – death.
One more point here: in addition to arguing from the data we don’t have, Isabella B pays insufficient attention to the data we do have when she states:
“For example, before the introduction of the measles vaccine in the US in the 1960s, there were “only” 400–700 measles deaths a year.”
For no year in the 1960s in the USA were 700 measles deaths recorded, nor 600, nor 500; 434 measles deaths in 1961 is the most yearly measles deaths recorded in the USA in the 1960s. The last year with close to 700 measles deaths recorded in the USA was 1951 with 683 measles deaths (See page 3 of the 2015 CDC Pink Book’s Appendix E).
The section under “Numerous factors affect mortality rates” is unclear but contains probable: projection, doubles down on misdirection, has a false premise, and an improbable and unsubstantiated implied premise
(Emphasis is from the original and is a subheading)
“Numerous factors affect mortality rates. Mortality rates are influenced by socioeconomic status, access to health care, quality of treatment and a wide range of other factors. As these factors change, mortality rates inevitably change. By contrast, as you can see from the graphs below, vaccine preventable disease incidence remained largely constant until the introduction of related vaccines. This may be because airborne diseases (like measles, mumps and rubella) can infect anyone, regardless of socioeconomic status.”
- Isabella B - Graphical Proof that Vaccines Work
It is not apparent what Isabella’s argument is here, but we can infer that since all the other arguments she provided are against those who “plot death rates over time” I will presume that she means this as an argument against looking at death rates and in favor of looking at incidence rates. Since Isabella was unclear here I can’t identify with certainty what she was doing or trying to do. I’m addressing this point of hers only because I promised a point by point deconstruction and this was apparently one of her points even if we can’t tell for sure what the point of it was. Here is my necessarily speculative deconstruction:
Projection: (accusing the other side of doing what your side is guilty of) Isabella acts as if she is setting the record straight by stating “Numerous factors affect mortality rates.” Well . . . who said otherwise? The Vaccine Apostates regularly point to nutrition, living conditions, water quality and so forth as probable reasons for the drastic decline in mortality that vaccines were not responsible for.
It is the Vaccinationists in particular who are guilty of ignoring other factors that affect mortality rates. As we saw with the exhibits of vaccine evangelism in the first installment of this series Part 1 – The Evangelists, the Evangelists repeatedly forgot other factors that affect mortality rates and simplistically credited vaccines as the primary player in reducing the mortality rates of infectious diseases.
Doubling Down on the Misdirection: Multiple factors affecting mortality rates does not change the fact that the death data is the relevant data source by which to evaluate the various vaccines save lives messages. No amount of notification of incident data will allow you to see if vaccines really did add 30 years to our lifespan as Paul Offit claims (see the Lifespan Lecture section of Part 1: The Evangelists, for four case examples of Paul Offit making that claim), but the death data will.
Isabella is likely continuing to judge death rate graphs on the premise that their principal purpose is to evaluate vaccine effectiveness rather than their usefulness for removing undue credit from vaccines by showing us what vaccines did not do. Isabella is continuing to fault the saw for not hammering nails.
False Premise: Isabella says “By contrast, as you can see from the graphs below, vaccine preventable disease incidence remained largely constant until the introduction of related vaccines.”
No it didn’t. Even if we assume that notification of incidence data is representative of actual incidence this statement of Isabella’s is untrue:
The polio incidence in the charts that Isabella provided by no means remains constant before the vaccine.
The diphtheria notifications of incidence was most certainly not constant before the toxoid vaccine she credits for it’s decline. This becomes clear when we ask the basic question when did widespread vaccination with diptheria toxoid actually begin? Which we will do shortly in my critical review of Isabella’s diphtheria graph.
Pertussis notifications certainly where not constant before the introduction of DTP vaccination as becomes clear in Isabella’s own graph when we correct the “misplaced” arrow as we will do in my critical review of Isabella’s pertussis graph.
Of all the graphs that Isabella herself provided only the measles and chickenpox notifications graphs, support Isabella’s assertion that “incidence remained largely constant until the introduction of related vaccines.” The other graphs either directly contradict her assertion, or do not contain enough pre-vaccine data to be of any worth in arguing for or against her assertion.
Improbable and Unsubstantiated Implied Premise: Isabella by pointing out that multiple factors affect mortality rates seems to be implying that multiple factors do not affect incidence rates. That would be equivalent to stating that incidence rates are only affected by one factor as more than one factor would be multiple factors.
Why should we assume that incidence rates are affected by only one factor? I know of no reason to make that assumption. Isabella should have identified what the one factor is that affects incident rates (presumably to Isabella the one factor is vaccination), and she should have offered an argument or relevant citation demonstrating that incidence rates are affected by only one factor.
If on the other hand Isabella did not mean to imply that incidence rates are affected by only one factor, then there is no apparent point to this part of her article.
The section under “Mortality rates are not more accurate than morbidity rates” is based on misrepresentation of the opposing argument
(emphasis is from the original and is a subheading)
“Mortality rates are not more accurate than morbidity rates. Those opposed to vaccination often use the “disease diagnoses are inaccurate” argument as a reason to look at mortality data only. However, the mechanism by which a doctor’s diagnosis suddenly becomes accurate when a patient dies, when he or she was not competent at diagnosing the disease in the first place, is not explained. In fact, death certificates will often be based on preceding diagnoses. Furthermore, as other researchers have noted, disease cases are more likely to be accurate as death certificates were only standardized from the 1960s onward [2].” - Isabella B - Graphical Proof that Vaccines Work
Isabella has misrepresented the opposition’s position, presumably to make the Vaccine Apostates’ arguments easier to attack. In other words she created a strawman. Her misrepresentation does contain a grain of truth. Let’s look at the grain of truth first and then the misrepresentations.
The grain of truth in Isabella’s portrayal of why Vaccine Apostates value death data over incidence data is that it is true, and Vaccine Apostates, do point out, that mild cases of disease are often more difficult to diagnose than serious cases (which Isabella does not acknowledge). Mild cases of an illness being more difficult to diagnose makes intuitive sense, but we can also easily find documentation of this in the medical literature that mild cases can be especially difficult to diagnose: early on in this essay in the excerpt that I shared from the British Medical Journal of February 9th 1959 “Dr. R. M. McGREGOR (Hawick, Roxburghshire) noted concerning a recent measles outbreak;
“Indeed, many of the cases were sufficiently mild as to make diagnosis difficult.”
In the article Natural course of 500 consecutive cases of whooping cough: a general practice population study. D. Jenkinson the author notes in the conclusion;
“Most cases of whooping cough are relatively mild. Such cases are difficult to diagnose without a high index of suspicion because doctors are unlikely to hear the characteristic cough, which may be the only symptom.”
The matter of mild cases being difficult to diagnose (if that is, a doctor ever sees the mild case to begin with), is clearly one of many concerns which casts doubt on the validity of notifications of incidence data as a measure of actual incidence.
For death data on the other hand, it is reasonable to presume that most cases of a disease which were severe enough to be the suspected cause of death, probably were not so mild as to be difficult to diagnose! Not that we should invest too much trust in the cause of death data on this basis, but we should note that there are some diagnostic issues which would be a concern for incidence data more so then for death data.
That is the grain of truth in Isabella’s portrayal now let’s look at the misrepresentations.
The first misrepresentation in Isabella’s statement is the premise that Vaccine Apostates are only concerned with diagnostic validity as it relates to notifications of incidence; contrary to Isabella’s portrayal of Vaccine Apostates, Vaccine Apostates have long cast doubt on the validity of recorded causes of death too:
Alfred Russel Wallace, writing Vaccination a Delusion in 1898, devotes multiple pages to evaluating and ultimately casting doubt on the validity of what was written in many of the death certificates forming the basis of the death statistics – in particular he brings up information which indicates that vaccination status was recorded or not on death certificates in a biased fashion that favored belief in vaccines, and that doctors avoided implicating vaccines as the cause of death when there was good reason too implicate them. This isn’t to say that Alfred Russel Wallace discounted death data, only that he was cautious and wary regarding how it was collected and did not invest full faith in the word of doctors.
Bystrianyk and Humphries in Dissolving Illusions, likewise provide numerous historical quotes which serve as cautionary examples of how death data can be and was skewed in favor of vaccinations. Bystrianyk and Humphries, also do not use this as reason to discount death data, but as an example of how death data can be manipulated.
The second misrepresentation that Isabella B gives us is the impression that the Vaccine Apostates are concerned primarily with incompetence on the doctor’s part affecting the validity of the diagnosis, but the primary concerns of the Apostates are not the doctors’ competence or incompetence but rather:
Changes in the definition of the disease
Changes in case definitions
Changes in diagnostic criteria
Diagnosis bias (not incompetence, not nefarious motives, but bias)
Apostates charge that these concerns can drastically affect both reported cases and the recorded cause of death.
The third misrepresentation in Isabella’s portrayal is the impression that she has tackled the principle reason why the Vaccine Apostates value death data over notifications of incidence data. She accomplished this through a lie by omission. She omitted the following which are principal reasons (plural - there’s more than one) for why Vaccine Apostates value death data over notifications of incidence data:
Death data is more consequential.
Death data is more complete.
Death data is available for more places over greater stretches of time.
Death data is the relevant data source for evaluating the various lives saved claims made by the vaccine evangelists.
See the section of this essay Differences Between Mortality and Morbidity Data Revisited for more detail concerning each of these reasons.
Fails To Substantiate Strong Assertion
Isabella lays the foundation of what could potentially be developed into an argument in favor of notifications data over death data with the following specific claim:
“Furthermore, as other researchers have noted, disease cases are more likely to be accurate as death certificates were only standardized from the 1960s onward [2].” - Isabella B - Graphical Proof that Vaccines Work
This claim, if true, could be the beginning of an argument. In and of itself this claim of Isabella’s does not prove accuracy of incidence data over death data - by itself this claim is not even an indicator of that; there are several other points that would have to be true, and Isabella would have to demonstrate them, or at least acknowledge them and offer appropriate citations before this claim of hers could logically be considered an effective argument for what she intends it.
But why expound upon this before we have established the truthfulness of Isabella’s base claim to begin with? Is Isabella’s claim that “death certificates were only standardized from the 1960s onward” even true?
Presumably she would cite a source that is sufficient to substantiate her claim, so what is the source that she cited? Here is what she cited.
. . . A New York Times article? That’s it? Well let’s give her the benefit of the doubt and see what pertinent information we can find in the article (emphasis mine);
“The University of Pittsburgh researchers also looked at death rates, but decided against including an estimate in the journal article, largely because death certificate data became more reliable and consistent only in the 1960s, the researchers said.”
That is paragraph is the only statement of support for Isabella’s assertion, to be found in the New York Times article that she cites to substantiate it.
Isabella has supported her assertion that “death certificates were only standardized from the 1960s onward” by stating that “other researchers have noted.” This in turn she backed with nothing more than a newspaper article that says “the researchers said.” This is a weak citation; what do we have here? We have Isabella saying that someone is saying something, which she supports with an article that says “the researchers said.” . . . Woefully inadequate.
As Isabella put forth no effort to substantiate her claim with a serious citation nor did she argue her case on this matter, we are under no obligation to accept or disprove her claim.
Nevertheless, I was curious to see if I could find anything to confirm or disconfirm Isabella’s claim. The first place I looked was the research paper that the New York times article which she cited was about, this paper:
Contagious Diseases in the United States from 1888 to the Present
This paper makes no mention of this claim, nor any statement that even pertains to the claim “death certificates were only standardized from the 1960s onward.”
I scanned the paper’s 30 citations to see if any of them were about death certificates or at least papers that would be likely to discuss death certificates, and found nothing of promise.
I even downloaded the paper’s 62 page supplementary appendix and used the “search and replace” program to search the document for the words death certificate singular and plural, and there was nothing there.
I followed this with some general internet searches for Isabella’s claim that yielded nothing.
Then I went straight to the technical appendices of the Vital Statistics of the United States. These are some of the most (possibly the most) widely referenced US government documents providing national cause of death data.
The vital statistics documents contain information about the data itself. The forwards and technical appendices contain frank assessments of the strengths and weaknesses of the data, information on how the data is collected, and often times examples of the death certificates themselves.
If there were significant lack of standardization in death certificates pre-1960s, and this threatened the reliability of the data, then there should be mention and warning of this in the forwards and technical appendices of these document. Furthermore, if there were a major change in standardization of death certificates that occurred in the 1960s, we should find mention of this in post 1960s Vital Statistics documents when they are discussing the data from previous years.
The first volume I checked was the Vital Statistics of the United States for 1960 to see what they had to say about the death certificates from which the data was collected. In the Technical Appendix, Section 7 - 3, under the subheading Standard Certificates we find the following (emphasis mine).
“Standard certificates of death and fetal ‘death, issued by the National Vital Statistics Division, have served for many years as the principal means of attaining uniformity in the content of the documents used to collect information on these events. They have been modified in each State to the extent necessitated by the particular needs of the
State or by special provisions of the State vital statistics law. However, the certificates of most States conform closely in content and arrangement to the standard certificate.”
This is the year 1960, and they are saying that standard certificates had served for many years as the principle means of attaining uniformity, and that the certificates of most states conform closely to this standard. This is a pretty clear indicator that they already had a relatively high degree of standardization, or at least enough for “attaining uniformity” by 1960 and that this relatively high degree of standardization had already been in place for many years.
That certainly doesn’t compute with Isabella’s statement that “death certificates were only standardized from the 1960s onward.”
Then I checked the Vital Statistics of 1970 to see what mention they make of changes in death certificates in the previous decade . . . well, none; in the technical appendix they simply reiterate that standard certificates of death have served for many years for attaining uniformity and that most states conform closely to them.
I have given Isabella’s unsubstantiated claim far more careful consideration then it merited, and the only pertinent information I can find, in relevant documents, directly contradicts her claim. This claim of Isabella’s, unsubstantiated though it was, was no doubt an effective rhetorical move on her part, as it is unlikely that many readers would have even paused at this statement, let alone singled it out for careful evaluation.
6. Critical Review of Incident Graphs in “Graphical Proof that Vaccines Work”
Let’s take a closer look at two of Isabella’s graphs.
While notifications of incidence data is generally more favorable to the vaccines than is the death data, some notifications of incidence data is still simply not favorable to the vaccines.
Isabella attempted to twist some unfavorable data sets into something favorable for the vaccine, let’s look at how she did that: the two graphs from her article that I will critically review are the US diphtheria notifications graph, and the US whooping cough notifications graph.
The Diphtheria Graph
Figure 21

That, is Isabella B’s diphtheria notifications of incidence graph. Isabella B claims that;
“The diphtheria vaccine was introduced in 1923 and caused a rapid decline in cases and deaths.”
As usual Isabella gives us no link to what her source is for this claim. As I mentioned in Part 2: definitive answers on when, where, and to what extent diphtheria vaccines came into use are hard to come by, and the CDC itself releases conflicting statements on the matter.
Isabella B evidently has encountered the same difficulty, for she provides no citation and presumably she is unsure of the significance of the date 1923, because she does not identify on the graph what is supposed to have happened in 1923 – was the vaccine licensed then? developed? Did a major national immunization campaign begin then?
What information I can find does not indicate any usage other than experimental usage, and certainly not widespread usage, of diphtheria toxoid vaccine in the USA in 1923 (emphasis in the following quotations is mine):
“Beginning in the early 1900s, prophylaxis was attempted with toxin-antitoxin mixtures. Toxoid was developed around 1921, but was not widely used until the early 1930s. It was incorporated with tetanus toxoid and pertussis vaccine and became routinely used in the 1940s.”
-Page 52 of Epidemiology and prevention of vaccine-preventable diseases /
edited by William Atkinson, CDC, Department of Health and Human Services, 6th edition, published 2000.
“The key figure in developing the first efficacious and well-tolerated toxoid vaccines was the French investigator Léon Ramon of the Pasteur Institute. Ramon used both heat and formalin to generate a chemically modified toxin (which he termed anatoxin) with better properties than those of Glenny's toxoid in 1923. The French Academy of Medicine approved this vaccine for children in 1927. } . . . { France used diphtheria toxoid widely among children and tetanus toxoid among the military during the 1930s. The United States and most other industrialized countries followed suit during the course of the same decade, during which time diphtheria toxoid replaced toxin-antitoxin as the preferred form of the immunization for children. Tetanus toxoid also became a routine U.S. pediatric immunization after the licensure of the first combination product against diphtheria and tetanus in 1947.”
Baker, J., Katz, S. Childhood Vaccine Development: An Overview. Pediatr Res 55, 347–356 (2004).
So we can see that, immunization was attempted (CDC author’s own word choice) with toxin-antitoxins early in the 19th century, the toxoid was developed around 1921, improved upon in 1923, used in France in the early 1930s and sometime after that came into widespread use in the USA (in the 1930s according to some, 1940s according to others) with universal vaccination not occurring until after the introduction of a combined diphtheria tetanus vaccine (DT), licensed in 1947 according to the above source, then it would have been used in the DTP vaccine shortly thereafter.
This is a prime example of apologists employing the post hoc fallacy; the mere development of a toxoid vaccine in 1923 is treated by Isabella as reason enough to credit subsequent decline in deaths and cases to this vaccine. Critical considerations like identifying when enough people were actually getting the vaccine for it to – even in theory – have been a major contributor to the decline are skipped over entirely.
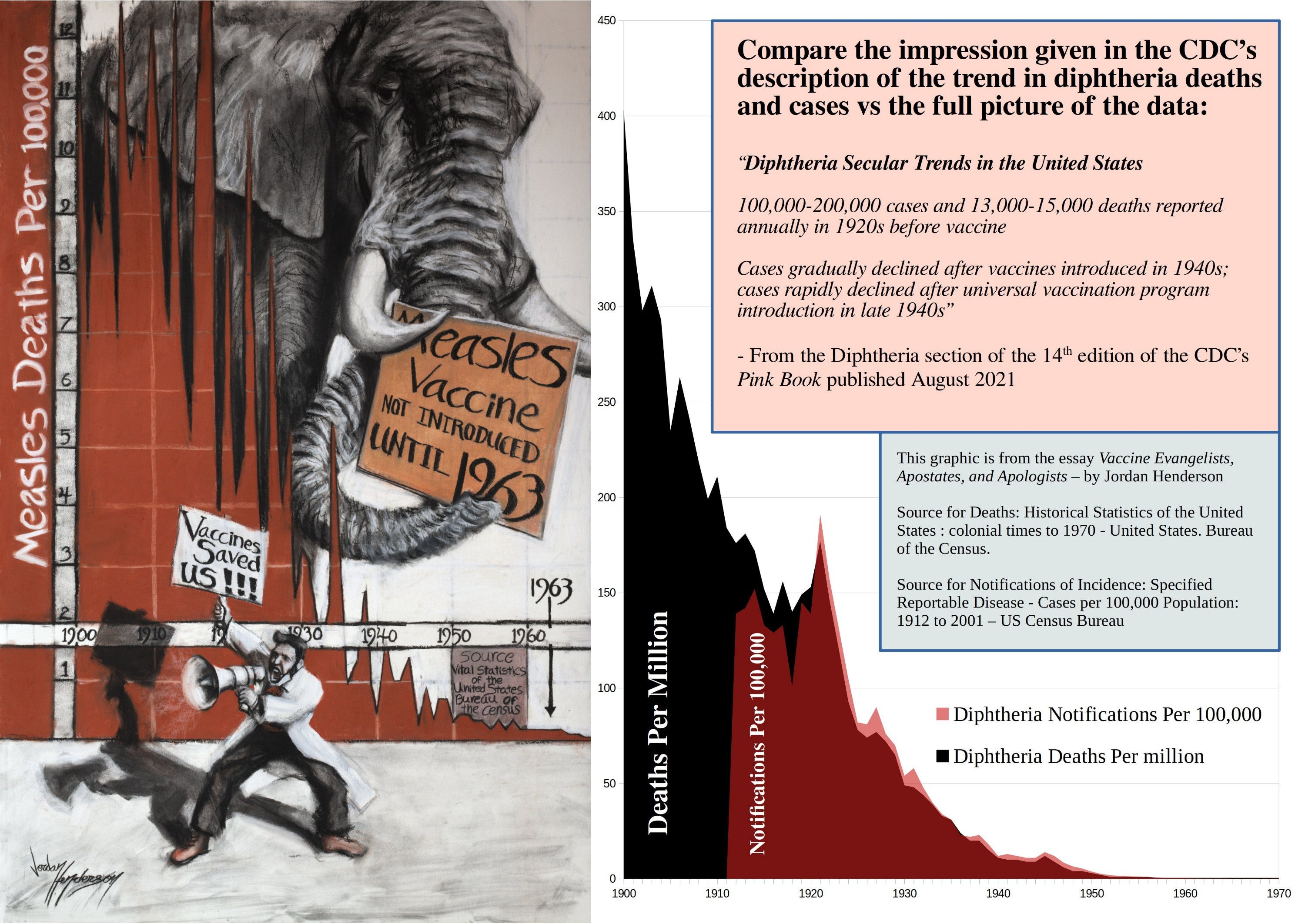
CDC Diphtheria Deception Revisited
In the second instalment of this essay series (Part 2: Apostasy) I shared the statement below from the CDC, which I noted was a classic example of Bait and Switch Preaching, and I also mentioned that the CDC is misleading us here on cases too.
“During the 1920s, 100,000 to 200,000 cases of diphtheria (140 to 150 cases per 100,000 population) and 13,000 to 15,000 deaths were reported each year. After diphtheria toxoid-containing vaccines became available in the 1940s, the number of cases gradually declined to about 19,000 in 1945 (15 cases per 100,000 population). A more rapid decrease began with implementation of a universal childhood vaccination program which included diphtheria toxoid-containing vaccines beginning in the late 1940s.”
- From the Diphtheria section of the 14th edition of the CDC’s “Pink Book” published August 2021
In the same section (Secular Trends in the United States [Referring to Diphtheria]) in the same pinkbook of the CDC they have an information box that says roughly the same thing but a little more clearly. They specify;
“Diphtheria Secular Trends in the United States
100,000-200,000 cases and 13,000-15,000 deaths reported annually in 1920s before vaccine
Cases gradually declined after vaccines introduced in 1940s; cases rapidly declined after universal vaccination program introduction in late 1940s”
- From the Diphtheria section of the 14th edition of the CDC’s “Pink Book” published August 2021
So let’s have some fun and juxtapose, the CDC’s statement about diphtheria and diphtheria vaccines with the data.
Figure 22
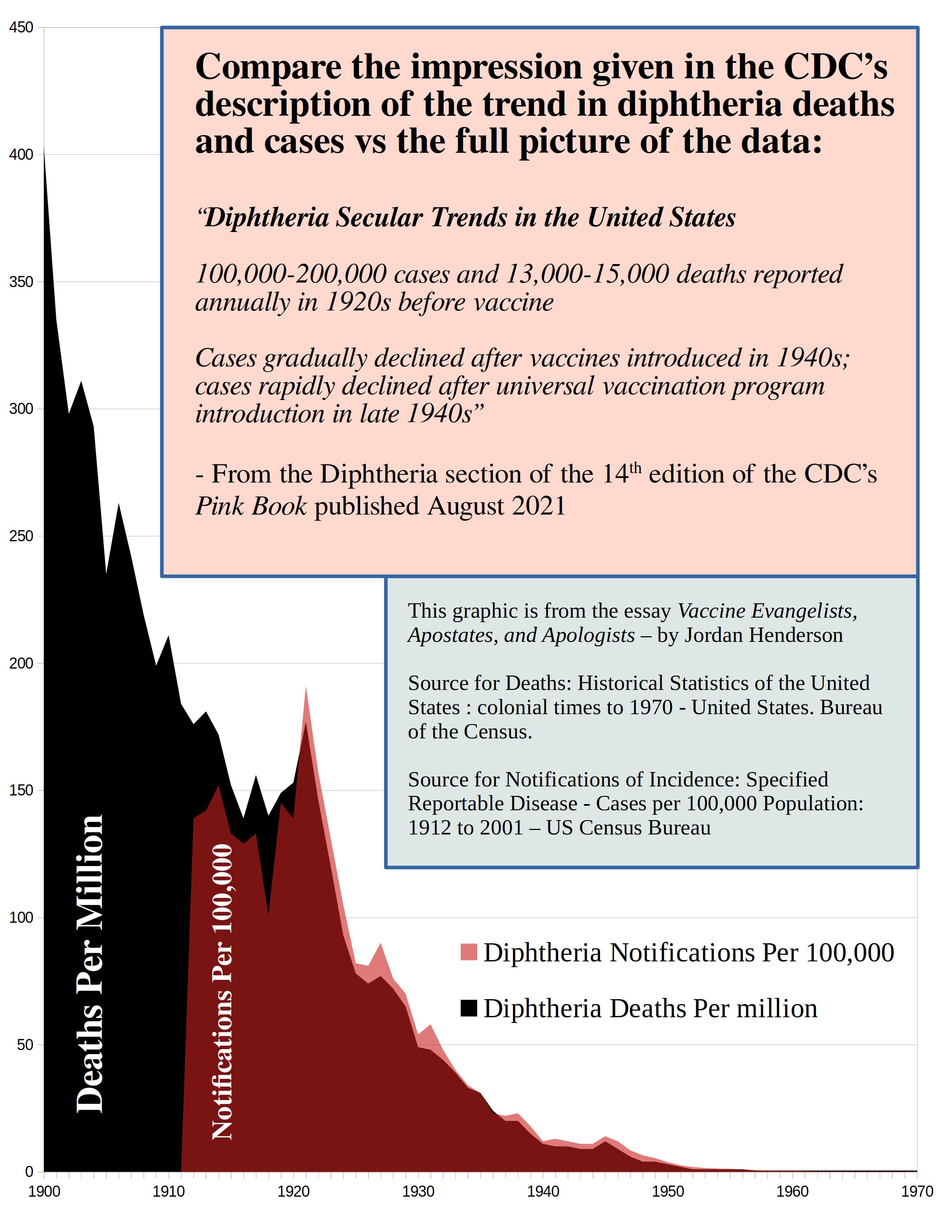
Here is the link to the source that I used for deaths in Figure 22, and here is the link for notifications.
You can now see clearly what I meant in the second instalment of this essay series (Part 2: Apostasy) about the CDC misleading us not just about diphtheria deaths, but that they were also misleading us concerning diphtheria notifications of incidence by giving us the impression that diphtheria cases began to decline in the 1940s after more widespread diphtheria immunization, when in reality the data shows the steep decline in the notifications rate as having begun decades earlier and probably most of the actual incidence decline occurring before the data was even available.
The excerpt we looked at earlier in this essay from the Vital Statistics of the United States – 1950 Page 63, Chapter 4, Notifiable Disease Statistics noted:
“On the other hand, a very high proportion of the potentially dangerous diseases such as smallpox, diphtheria, and typhoid fever, are reported.”
Unlike measles where incidence rates and death rates diverge to a very great degree, we can see that for diphtheria in the USA the notifications of incidence rate closely mirrors the death rate, at about ten notifications to each death.
So we should be able to get a tentative, rough estimate of diphtheria rates for the first decade of the 20th century by using the 10 to 1 cases to deaths ratio, and multiplying the death rate by ten to get the cases. If that’s reasonable methodology for this disease where the case rate and death rate closely mirrored one another, then we can estimate that the greater part of the 20th century decline in diphtheria cases occurred before 1912.
Clearly the US historical data sets for diphtheria deaths and incidence are both unfavorable to the vaccinationist’s narrative. The probable reason for why the 20th century US diphtheria notifications data isn’t quite as unfavorable to the vaccinationists as is the death data is simply because the first 12 years of it are missing.
The Pertussis Graph
Returning to Isabella B’s Graphical Proof that Vaccines Work let’s look at the Pertussis graph she provided.
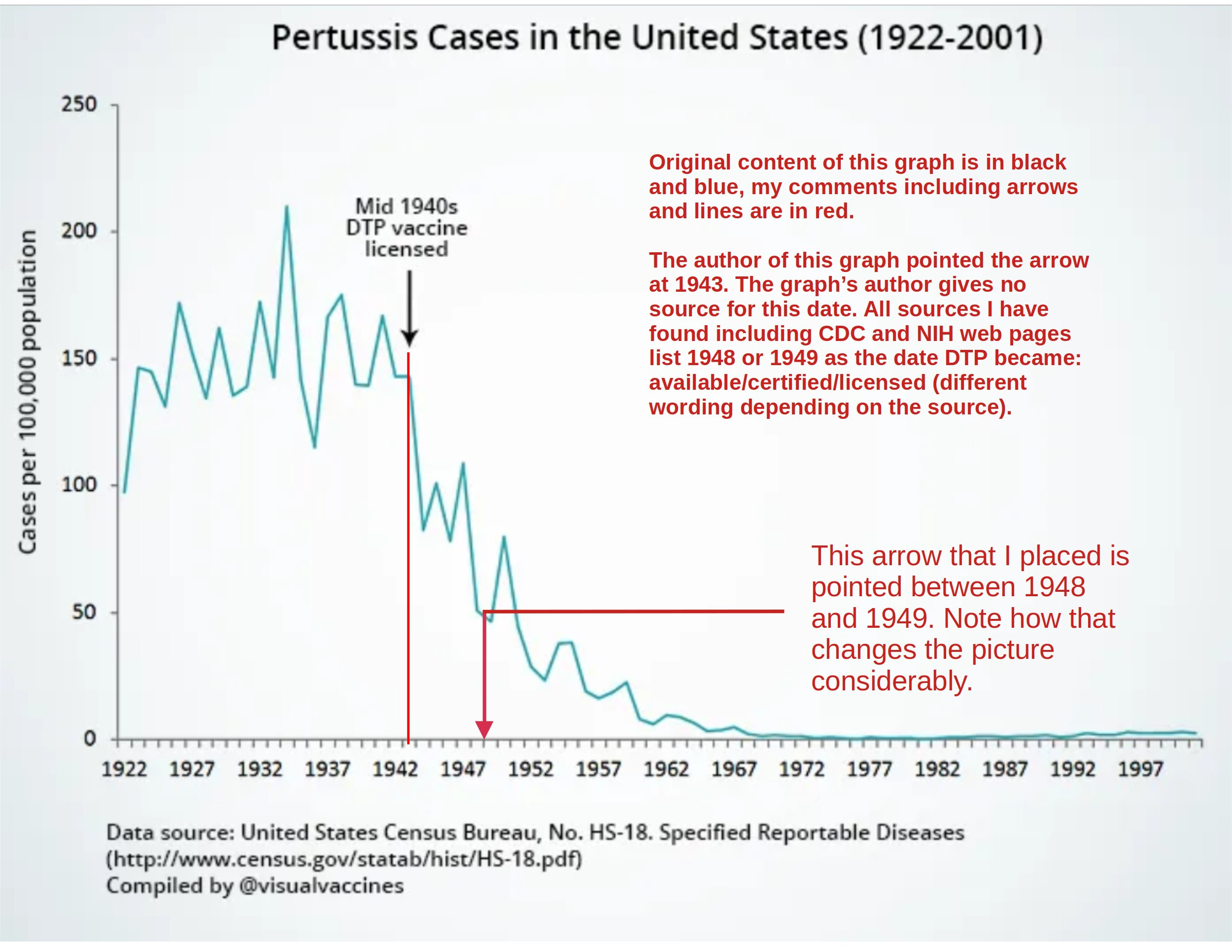
Figure 23

Firstly we note just how little pre-vaccine pertussis notification data there is; it only takes us back to 1922. That’s not Isabella’s fault, that data is just not available, but it does underscore one of several reasons for why incident notification data is less useful – much of it is missing.
Secondly, Isabella’s graph says “Mid 1940s DTP vaccine licensed” with an arrow pointing to 1943. She gives no source for this as usual. All sources that I have found point to DTP being available in 1948 and licensed in either 1948 or 1949.
The CDC pinkbook, and published papers like this one, or this one say DTP became available in 1948. This paper says it was licensed in 1948.
Immunize.org says DTP was licensed in 1949. The History.NIH.gov website says DTP became available 1948 and was certified in 1949.
The Texas Department of Health Services under Licensure Dates for Vaccines and Toxoids, United States lists 1949 as the year DTP was licensed in the US.
So unless everyone including multiple government agencies are totally off the mark then DTP was introduced/certified/licensed in 1948 and/or 1949. Let’s correct the arrow placement and see how that changes the picture.
Figure 24
Correcting the arrow placement changed the picture to such a degree as to turn this notifications of incidence data set from one that looked favorable to the vaccinationists claims about the DTP vaccine into a data set that is unfavorable to their claims.
The CDC “misplaces” arrows too, in a way that makes this data set look better for the DTP vaccine.
Figure 25
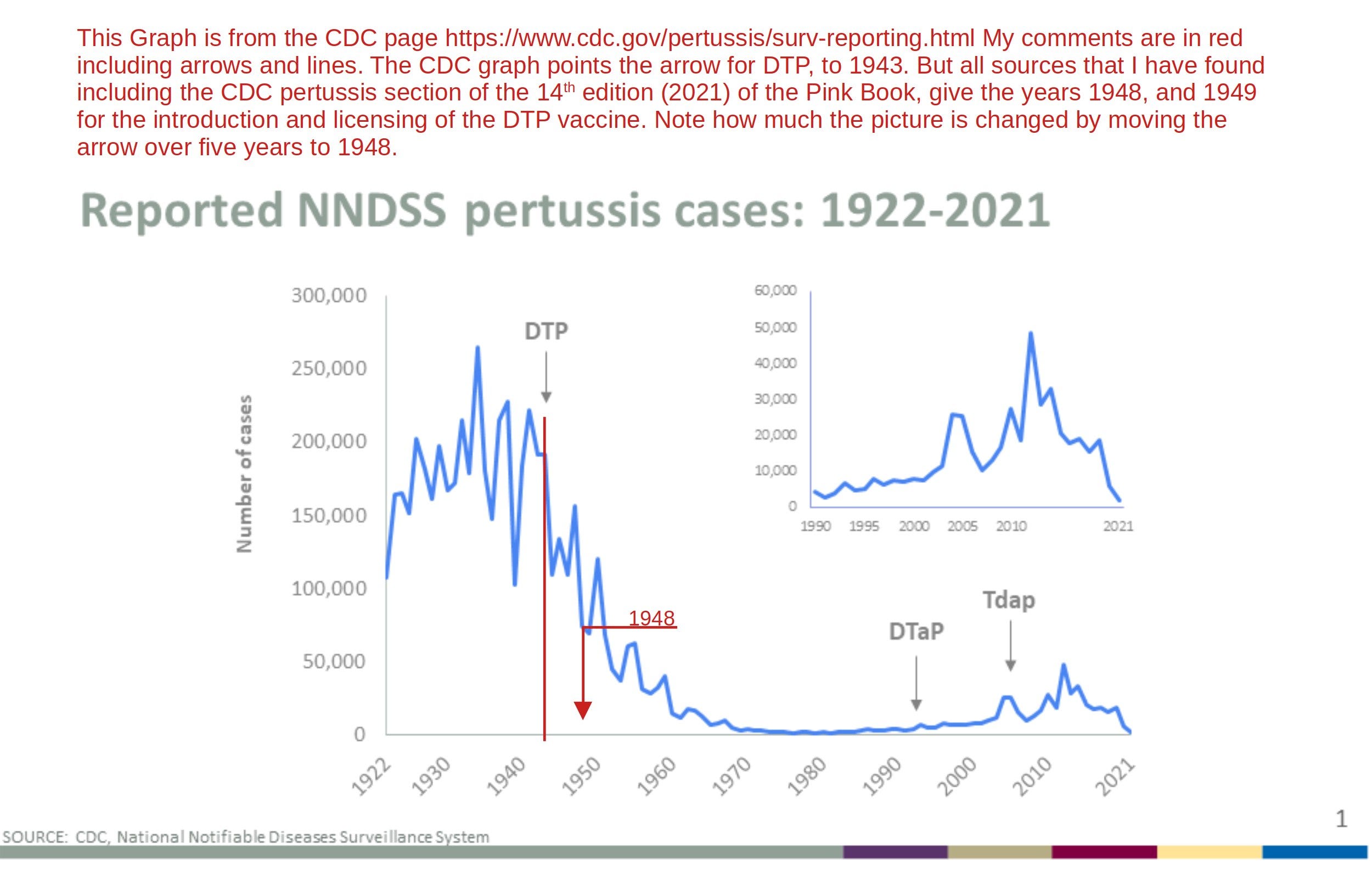
The CDC graph in Figure 25 is from this web page at the CDC. Despite it being difficult to tell with precision which peak and which trough correspond to which year from the CDC’s graph, we can figure that out by consulting the data table that the chart is based on, which is what I did.
We shouldn’t get too excited about correcting the arrow placement on these graphs though; For the vaccinationists a vaccine just needs to exist, and that’s reason enough to credit any decline in deaths and incidence from then on to the vaccine.
There were some pertussis vaccines being developed and used here and there in the US before the DTP vaccine; no doubt our vaccinationist friends would simply give any credit they can’t give to the DTP vaccine to its precursors if these graphs with corrected arrow placement were brought to their attention. Whether or not enough people actually even got those early pertussis vaccines for them to plausibly be credited for much of anything at the national level is not the sort of detail they would allow to get in their way.
This concludes my deconstruction of Isabella B’s Graphical Proof that Vaccines Work. There are some loose ends of course: I did not address the polio graphs she created, or the claims about them that she made; for Vaccine Apostate takes on the official polio mythology I offered some recommended reading at the end of the second installment of this essay series (Part 2: Apostasy) which I refer back to for those who would like to delve into polio.
For a fine heretical take on Hib (which Isabella provided graphs of) I recommend Greg Beattie’s book Fooling ourselves on the fundamental value of vaccines (in particular - Chapter Six INVENTING NEW DISEASES).
However, no need to be greedy; we covered a lot of ground in this deconstruction and this tour of the Motte. Familiarity with death vs notification of incidence data is critical to understanding the debate surrounding the undue credit given to vaccines. With this essay we’ve laid some very important groundwork and we began the deconstruction of the Apologists earlier then initially planned. We’re working ahead of schedule. Let’s briefly review the Red Herring side of the Motte and then we’re done for now (till the next essay installment that is, Part 4: Spanish Death Data.)
4. Conclusion: The Motte is a Red Herring
The red herring analogy - A red herring is a pungent smoked fish. The analogy of a red herring is based on the idea of distracting a hound that is after a rabbit by dragging this pungent smoked fish (the red herring) across the scent trail of the rabbit with the intent to redirect the hound away from the rabbit by encouraging it to pursue the red herring instead.
When Vaccine Apologists make the switch to notifications of incidence data, they are not just retreating into a more defensible area (their Motte), they are redirecting the conversation away from the sensitive issue that the death data contradicts the Vaccine Evangelist’s preaching.
The rabbit is the Vaccine Evangelists preaching their Graveyard Gambits, Bait and Switch Preaching, Lifespan Lectures, and all manner of Vaccines Save Lives messages for which death data is the relevant data source by which to evaluate the Evangelist’s claims.
The hound pursuing the rabbit is the Vaccine Apostates who are debunking the Vaccine Evangelist’s preaching through death data (among other evidences).
The red herring is the notification of incidence data, which the Vaccine Apologists are dragging across the scent trail with the intent of diverting the conversation away from the death data. The Apologists act as if there never was a rabbit to begin with (act as if the Vaccine Evangelists had never been promoting the misconceptions that they are still actively promoting).
For example; almost the entire written portion of Isabella B’s article was devoted to arguing that death data wasn’t the appropriate data source and that we really should be looking at notifications data instead.
Isabella gave us no documentation of who she was criticizing, which left her free to portray the opposition as she pleased without real world examples getting in the way. She dismissed death rate graphs with the this saw is no good because it doesn’t hammer nails type of reasoning. Isabella attempted to downplay the worth of death data by employing the argument from the data we don’t have. The written portion of Isabella’s article was one great big act of dragging a red herring across the trail, and getting the attention away from the death data (save for the few favorable death data sets which Isabella suddenly found appropriate to look at).
We will deconstruct many more case examples of Vaccine Apologetics, in Part 6: The Apologists and in an Appendix. When we do, watch for this strategy; these works of vaccine apologetics are almost all acts of dragging a red herring across the trail. They all reroute the conversation away from death data using variations of the strategies that Isabella employed. The skillfully executed retreats into the Motte like Isabella’s article, leave the unwary reader focused on the red herring and forgetful of there ever having been a rabbit.
A Couple Ideas for Those Who Would Like to Support This Work
To those who would like to support my work, I offer the following three suggestions, any one or combination of which would be most helpful:
1. Making a small single, or recurring donation to me through the donation page on my website (or a paid Substack subscription which is effectively a donation as all my essays are freely available), or making a purchase of a small print, mug, or greeting card, through my art prints website.
2. Making a single or recurring donation to one of the independent media outlets who publish my work, and without whom few would see my work online to begin with.
3. Supporting this work by getting the word out; sharing this article, and or sharing other notable works by me or the independent media outlets who bring my work to your attention. This increases our reach and makes us happy to know that our work is benefiting more people.
Up next: Part 4 – Spanish Death Data
In the next essay we expand our knowledge of pre-vaccine declines in infectious disease mortality by reviewing a century of readily available death, and vaccines-administered data from Spain.
→ Read Part 4: Spanish Death Data
Jordan Henderson lives in Washington State in the Northwest of the United States. He works in oil paints, and charcoals. A portfolio of his works can be viewed at either of his websites: Original Paintings – Fine Art Prints